Author Positionality Statement
Nickol Georgy and Circe Gray Le Compte, ScD, MS, come to this analysis from distinct disciplinary, institutional, and life-stage positions, and we recognize that these positions shape the questions we ask of the data and the interpretations we bring to the results. Nickol is an undergraduate researcher at the University of Southern California majoring in Quantitative Biology and minoring in Applications of Artificial Intelligence. She is affiliated with the Bionic Ear Lab, where her work examines the sociological dimensions of hearing loss and the development of computational tools to reduce background noise for cochlear implant users. She approaches this analysis as an emerging quantitative scholar oriented toward justice, with a particular interest in how administrative data can illuminate, but also flatten, the lived realities of patients moving through U.S. health systems. Her positionality informs the analytic emphasis on structural drivers of care-seeking and the rejection of individualist framings of avoidable ED utilization.
Dr. Le Compte is a Harvard-trained social epidemiologist with extensive experience in theoretical and applied research, evaluation, and communications experience in public health, with sustained focus on HIV, aging with HIV, LGBTQ+ health, harm reduction, and the structural and social determinants of health inequity. She is co-CEO of BCPH, the publisher of BCPHR, and has held leadership and research roles with NMAC (formerly the National Minority AIDS Council), HealthHIV, and Impact Marketing + Communications, as well as postdoctoral fellowships at Columbia University and Rutgers University. Her positionality is shaped by long engagement with community-based and community-accountable research on medically complex and structurally marginalized populations, and by the conviction that access architecture, rather than patient behavior, is the appropriate frame for understanding most patterns of emergency care use.
The authors approach research, analysis, and dissemination as collaborative and accountable processes. They recognize that they are studying populations whose lived experiences exceed what administrative data can capture, including patients navigating immigration enforcement, chronic and complex illness, behavioral health needs, disability, primary care deserts, and predatory medical financing. They acknowledge that we do not hold all of the identities represented in the populations described in this analysis, and that their disciplinary training, institutional affiliations, career stages, and personal histories shape the questions they have chosen to ask of these data and the structural interpretive lens they apply. They have framed their interpretations to avoid pathologizing care-seeking patterns that emerge from structural constraints, to center patients’ strategic logic, and to produce work that is methodologically rigorous, transparent about its limitations, and useful to the communities most affected by the access architecture their analysis describes.
Background
Emergency department (ED) visits classified as avoidable, in which patients seek care for non-emergent conditions that could be managed in primary care or ambulatory settings, remain a persistent and costly feature of the United States health care system.1–3 National estimates indicate that 5% to 40% of ED visits may be classified as avoidable depending on the methodology used, with urban centers reporting rates at the upper end of that range.4–7 Avoidable ED utilization contributes to overcrowding, ambulance diversion, longer wait times for time-sensitive conditions, workforce burnout, increased left-without-being-seen rates, and worse downstream outcomes for patients with genuine emergencies.8–14 Reducing avoidable ED visits is therefore a long-standing priority for payers, hospitals, and state health systems, as well as a recurring focus of national equity frameworks such as Healthy People 2030.15
A common assumption in policy and clinical discourse is that publicly insured and uninsured patients drive avoidable ED utilization because they face greater barriers to primary care access.16–20 The reality is more contested. Studies of the Affordable Care Act (ACA) Medicaid expansion produced mixed evidence: some analyses showed increased ED visits following coverage expansion,21,22 while others reported no change or modest reductions in avoidable use, particularly among young adults.23–25 Cross-sectional studies have variably found that Medicaid and uninsured populations exhibit higher17,26,27 or lower28,29 rates of avoidable ED utilization than the privately insured, with effect sizes that depend strongly on the operationalization of avoidability and the inclusion of clinical adjustment. Lack of usual source of care, limited after-hours primary care access, and transportation barriers are recurrent structural drivers across these studies.28–31 A central insight from the Agarwal et al. exploration of insurance status and ED utilization is that the relationship is not a simple coverage-versus-access calculus but is shaped by the structural availability of alternatives, the clinical complexity of the population, and the cultural and economic contexts of care-seeking.26
Recent empirical work using statewide hospital discharge data in New York found a pattern that runs counter to the conventional narrative: relative to privately insured patients, publicly insured patients had 14% lower adjusted odds of avoidable ED visits, and uninsured patients in the Self-pay/Miscellaneous/Other category had 12% lower odds.18 These findings, derived from a multinomial logistic regression with insurance as the outcome and severity of illness as a predictor, challenge conventional narratives about Medicaid overuse and raise the question of which clinical and socioeconomic factors structure the observed association. Comparable patterns have been described in other settings, including Florida-based ambulatory-care-sensitive condition (ACSC) analyses27,32 and English national studies of preventable emergency care,33 suggesting that the New York finding is not anomalous but reflects broader structural dynamics. The growth of avoidable ED use among privately insured Americans has been documented for two decades, beginning with Cunningham and May’s national tracking study34 and confirmed by Pukurdpol and colleagues’ analysis showing that primary-care-treatable ED visits had increased disproportionately among publicly insured populations only after baseline coverage equalization, leaving the privately insured as a persistent locus of non-emergent ED use.17
The objectives of the present study are to characterize the demographic, geographic, and clinical correlates of insurance type and to estimate the adjusted association between insurance type and avoidable ED visits in New York State during 2022, with explicit attention to the structural mechanisms (primary care deserts, specialty referral barriers, immigration enforcement, chronic disease complexity) that shapes care-seeking among populations whose strategic decisions are too often misread as passive overuse.
The present study extends prior work in three respects. First, it specifies avoidable ED visit as the binary outcome and insurance type as the primary exposure, providing more direct interpretation of the policy-relevant relationship. Second, it incorporates richer clinical adjustment, including the APR Major Diagnostic Category for the principal diagnosis, the type of admission, and the medical/surgical care designation, which capture diagnostic mix more comprehensively than severity and risk of mortality alone.35–39 Third, it uses the full available analytic sample of ED-related discharges among adults to maximize statistical precision. The objectives are to characterize the demographic, geographic, and clinical correlates of insurance type and to estimate the adjusted association between insurance type and avoidable ED visits in New York State during 2022, with explicit attention to the structural mechanisms (primary care deserts, specialty referral barriers, immigration enforcement, chronic disease complexity) that shape care-seeking among populations whose strategic decisions are too often misread as passive overuse.
Theoretical Framework
This analysis is grounded in two complementary theoretical traditions. The first is Andersen’s Behavioral Model of Health Services Use, which organizes the determinants of care-seeking into predisposing factors (demographics, social structure, health beliefs), enabling factors (insurance, income, geographic access), and need factors (perceived and clinically evaluated illness).40,41 The model has been the dominant framework for ED utilization research for half a century and provides a parsimonious vocabulary for distinguishing whether observed insurance differences operate through predisposition, enablement, or clinical need.
Krieger’s ecosocial theory of disease distribution further refines our theoretical lens, focusing on population health patterns as embodiments of historically and politically structured exposures, with attention to who and what is responsible for inequities and at what level of the social-ecological system.42 Where Andersen’s framework specifies the proximal mechanisms through which insurance type translates into ED use, ecosocial theory contextualizes those mechanisms within the political economy of US health care: the geography of primary care supply, the architecture of insurance benefits, the legal frameworks that govern access, and the immigration and policing regimes that determine who feels safe seeking care.43
Together, these frameworks reframe avoidable ED utilization away from individual-level “overuse” or “misuse” narratives and toward a structural reading. Patients are not passive consumers but strategic actors who weigh the constraints of their insurance benefit design, the supply of accessible primary care, the friction of specialty referral, the risk of immigration enforcement or surveillance in formal health care settings, and the financial consequences of uninsured care, including exposure to predatory medical credit products.44,45 The Andersen-ecosocial integration motivates the inclusion of geographic context (NYC versus outside NYC), diagnostic complexity (APR MDC), and clinical severity in the analytic model, and motivates the structural interpretation we apply to the results in the discussion.
Methods
Data Source and Study Design
This was a retrospective cross-sectional analysis of de-identified 2022 inpatient discharge data from Health Data New York’s Statewide Planning and Research Cooperative System (SPARCS), specifically the publicly available file titled “Hospital Inpatient Discharges (SPARCS De-Identified): 2022,” last updated April 1, 2025.46 SPARCS is an all-payer reporting system maintained by the New York State Department of Health that captures discharge information from hospitals across the state. The dataset contains 33 variables covering patient demographics, diagnoses, services, and charges. Because the data are publicly available and fully de-identified, this analysis was deemed exempt from institutional review board oversight.
Study Population and Analytic Sample
From the full 2022 file (n = 2,103,433 inpatient discharges), we restricted analysis to records flagged as ED-related (Emergency Department Indicator = “Y”), yielding 1,337,271 discharges. We further restricted to adults age 18 and older and excluded records with missing data on the outcome, primary exposure, or any covariate included in Model 1. The final analytic sample comprised 1,258,855 ED-related adult discharges.
Outcome
The outcome was avoidable ED visit, a binary indicator derived from the APR Severity of Illness variable. Records classified as Minor severity were coded as 1 (avoidable), and records classified as Moderate, Major, or Extreme severity were coded as 0 (non-avoidable). This operationalization is consistent with prior SPARCS-based research18 and with the assumption that minor-acuity conditions are typically appropriate for primary or ambulatory care rather than the ED. Alternative operationalizations, such as the New York University ED algorithm35,36 and machine-learning classifiers trained on the National Hospital Ambulatory Medical Care Survey,37 were not used because they require diagnostic-code-level inputs not consistently coded in the de-identified SPARCS file.
Primary Exposure
Insurance type was constructed from the SPARCS Payment Typology 1 variable and categorized into three groups: Private (Private Health Insurance, Blue Cross/Blue Shield, Managed Care Unspecified); Public (Medicare, Medicaid, Federal/State/Local/VA); and Uninsured (Self-pay, Miscellaneous/Other). Private insurance served as the reference category in all regression models. The Uninsured category as constructed here may include both fully uninsured patients and those whose payment typology was incomplete or miscellaneous; this limitation, common to administrative discharge data, is discussed below.
Covariates
Demographic covariates included age group (18 to 29, 30 to 49, 50 to 69, 70 and older), sex (Male, Female), race (White, Black/African American, Multi-racial, Other Race), and Hispanic ethnicity (Not Hispanic, Hispanic, Unknown). Geographic context was captured by hospital service area, dichotomized as New York City versus outside New York City. Clinical covariates included length of stay (1 day, more than 1 day), APR Risk of Mortality (Minor, Non-minor combining Moderate/Major/Extreme), care type (Medical, Surgical), type of admission (Emergency, Non-emergency), and the APR Major Diagnostic Category for the principal diagnosis. The MDC variable was collapsed into 11 categories: Circulatory, Respiratory, Infectious and Parasitic, Digestive, Nervous, Musculoskeletal, Kidney/Urinary, Mental Health, Pregnancy/Childbirth, Substance Use, and Other (reference). Although the AHRQ Elixhauser comorbidity index39 would have provided a finer-grained adjustment for comorbidity, comorbidity-level variables were not available in the public-use file.
Statistical Analysis
Descriptive statistics were calculated for all study variables, with cross-tabulations and chi-square tests examining associations between covariates and insurance type. Two principal logistic regression models were estimated with avoidable ED visit as the binary outcome. Model 0 was an unadjusted bivariate logistic regression of avoidable ED on insurance type. Model 1 was a fully adjusted multivariable logistic regression that included all covariates simultaneously, including the full APR Major Diagnostic Category. To enable a clean test of effect modification by mental health diagnosis, we additionally estimated Model 1B, which retained all demographic, geographic, and severity covariates but replaced the 11-category MDC variable with two binary indicators: a mental health diagnosis indicator (APR MDC: Mental Diseases and Disorders) and a substance use diagnosis indicator (APR MDC: Alcohol/Drug Use and Alcohol/Drug Induced Organic Mental Disorders).18 Adjusted odds ratios (AORs) and 95% confidence intervals (CIs) were derived by exponentiating regression coefficients. Model fit was assessed using the McFadden pseudo R-squared, the log-likelihood, and the likelihood ratio test against the null model. Analyses were conducted in Python 3.12 using the statsmodels library. Statistical significance was set at p < .05 (two-sided). (See a summary of analytic models in Table 1.)
Effect Modification
We tested whether the relationship between insurance type and avoidable ED utilization was modified by mental health diagnosis using two complementary approaches. First, we estimated an interaction model (Model C) by adding insurance-by-mental-health interaction terms to Model 1B and tested their joint significance with a likelihood ratio test against the no-interaction model. Second, we re-estimated Model 1B separately within strata defined by the presence or absence of a mental health diagnosis. Stratified estimation provides directly interpretable AORs within each subgroup and is robust to interpretive complications that arise when interaction terms produce non-monotonic effects on the odds ratio scale.
Sensitivity Analyses
We conducted four sensitivity analyses to test the robustness of the primary findings. First, we reclassified the SPARCS Managed Care, Unspecified payment typology from Private to Public, since some Managed Care plans operate as Medicaid managed care. Second, we disaggregated the Uninsured category into separate Self-Pay and Miscellaneous/Other groups, since the original construction may pool patients with materially different financial circumstances. Third, we estimated stratified models by age (under 50 versus 50 and older) to assess whether the association between insurance type and avoidable ED visits varies across the life course in ways not captured by the age-group covariate. Fourth, we estimated stratified models by hospital service area (NYC versus outside NYC) to assess whether the association varies across geographic context with different primary care supply, immigration density, and safety-net infrastructure.
Results
We organize the results in four blocks: sample composition, the unadjusted (crude) association between insurance type and avoidable ED visits, the fully adjusted association, and the broader pattern of correlates revealed by Model 1, including age-stratified subgroup patterns. Each block builds on the previous one and informs the structural interpretation developed in the Discussion.
Sample Characteristics
Descriptive characteristics of the analytic sample, overall and stratified by insurance type, are presented in Table 2. Among 1,258,855 ED-related discharges, 79.8% were covered by public insurance, 18.0% by private insurance, and 2.2% were uninsured. Avoidable ED visits accounted for 18.3% of all encounters, with substantial variation by insurance type: 28.3% among privately insured, 27.9% among uninsured, and 15.8% among publicly insured patients. The publicly insured group was older (49.6% age 70 and older) than the privately insured group (7.7%) or the uninsured group (18.2%). Compared with privately insured patients, publicly insured patients were more likely to be Hispanic (15.7% vs 11.0%), to receive care in New York City facilities (45.2% vs 41.3%), and to have non-minor risk of mortality (71.0% vs 48.9%). Uninsured patients were disproportionately male (64.8%), younger (47.4% under age 50), and more likely to have musculoskeletal diagnoses (18.1% vs 5.7% among privately insured), patterns consistent with prior characterizations of the uninsured ED population in safety-net contexts.47–49 All bivariate associations between covariates and insurance type were statistically significant (p < .001), reflecting the large sample size.
Having established the demographic and clinical contours of the sample, we next assess the unadjusted relationship between insurance type and avoidable ED classification, which establishes the baseline pattern that motivates the multivariable analysis.
Crude Association Between Insurance Type and Avoidable ED Visits
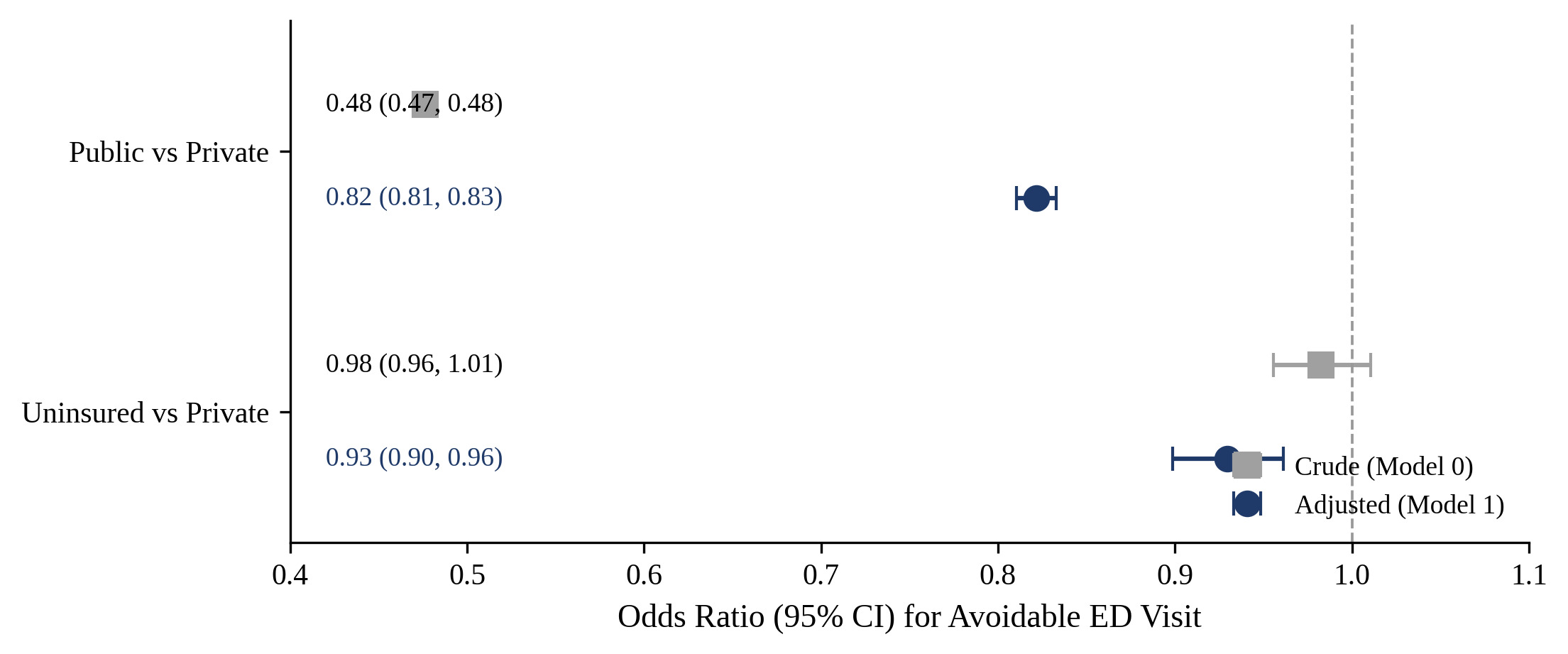
In the unadjusted bivariate analysis (Model 0), public insurance was strongly associated with lower odds of avoidable ED visits relative to private insurance (OR = 0.48, 95% CI: 0.47, 0.48, p < .001). The crude association for the uninsured group was not statistically significant (OR = 0.98, 95% CI: 0.96, 1.01, p = .221). These crude estimates reflect the combined influence of insurance type and the demographic and clinical factors that covary with it, including the predominance of older adults and patients with non-minor risk of mortality in the publicly insured group. Because these crude differences may reflect confounding by age, severity, diagnostic mix, and other factors that vary by insurance type, we next estimate fully adjusted models to examine whether the public and uninsured patterns persist after accounting for these covariates.
Adjusted Association Between Insurance Type and Avoidable ED Visits
In the fully adjusted Model 1, the association between insurance type and avoidable ED visits attenuated substantially but remained statistically significant in the same direction. Compared with privately insured patients, publicly insured patients had 18% lower adjusted odds of avoidable ED visits (AOR = 0.82, 95% CI: 0.81, 0.83, p < .001). Uninsured patients had 7% lower adjusted odds compared with privately insured patients (AOR = 0.93, 95% CI: 0.90, 0.96, p < .001), an effect that emerged only after adjustment. Crude and adjusted odds ratios are presented in Table 3 and visualized side by side in Figure 1.
_and_adjusted_(model_1)_odds_ratios_for_the_association_between_insurance_t.png)
The marked attenuation of the public-insurance estimate from OR = 0.48 to AOR = 0.82 indicates that approximately two-thirds of the crude association is accounted for by the demographic and clinical variables included in Model 1, particularly age and risk of mortality. The remaining adjusted association suggests that the lower probability of avoidable ED visits among publicly insured patients is not fully explained by their older age or higher clinical complexity, a finding consistent with prior reports that age and severity adjustment do not fully eliminate insurance-related differences in non-emergent ED use.18,27,28 To clarify how other demographic and clinical characteristics structure avoidable ED classification, and how insurance operates within those strata, we next examine the full set of Model 1 predictors and then explore age-stratified patterns.
Other Correlates of Avoidable ED Visits
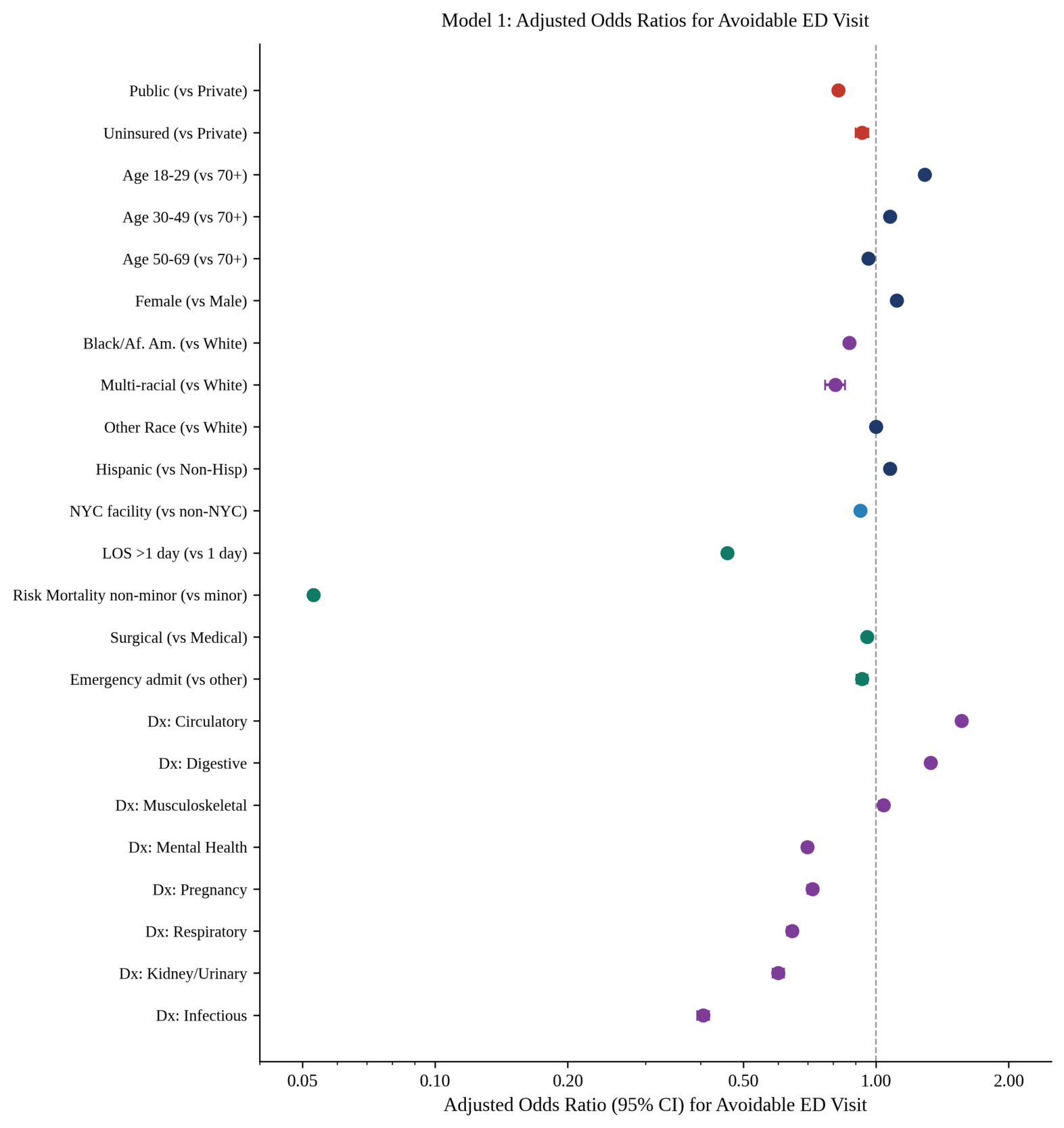
Adjusted odds ratios for all Model 1 covariates are presented in Table 4 and visualized as a forest plot in Figure 2. Younger age was strongly associated with higher odds of avoidable ED visits, with adults aged 18 to 29 showing 29% higher adjusted odds compared with adults age 70 and older (AOR = 1.29, 95% CI: 1.26, 1.32, p < .001), consistent with national patterns of higher non-emergent ED use among younger adults.7,49 Female sex was associated with 12% higher adjusted odds (AOR = 1.12, 95% CI: 1.10, 1.13, p < .001). Compared with White patients, Black/African American patients had lower adjusted odds of avoidable ED classification (AOR = 0.87, 95% CI: 0.86, 0.88, p < .001), as did multi-racial patients (AOR = 0.81, 95% CI: 0.77, 0.85, p < .001), patterns that may reflect later presentation, higher acuity at presentation, or differences in severity coding rather than lower overall ED use.27,50 Hispanic ethnicity was associated with modestly higher adjusted odds (AOR = 1.08, 95% CI: 1.06, 1.10, p < .001). Care delivered in New York City facilities was associated with 8% lower adjusted odds (AOR = 0.92, 95% CI: 0.91, 0.93, p < .001).
Clinical severity covariates showed the largest effects in the model. Length of stay greater than one day was associated with 54% lower adjusted odds of avoidable ED classification (AOR = 0.46, 95% CI: 0.45, 0.47, p < .001), and non-minor risk of mortality was associated with 95% lower adjusted odds (AOR = 0.05, 95% CI: 0.05, 0.05, p < .001). These very large effects are expected given that risk of mortality and severity of illness, both APR-derived constructs, share common clinical inputs. Diagnostic category effects were also substantial: relative to the Other category, circulatory diagnoses (AOR = 1.56, 95% CI: 1.53, 1.59, p < .001) and digestive diagnoses (AOR = 1.33, 95% CI: 1.30, 1.36, p < .001) were associated with higher odds of avoidable classification, whereas infectious diseases (AOR = 0.41, 95% CI: 0.39, 0.42, p < .001), respiratory conditions (AOR = 0.65, 95% CI: 0.63, 0.66, p < .001), kidney and urinary conditions (AOR = 0.60, 95% CI: 0.58, 0.62, p < .001), and mental health conditions (AOR = 0.70, 95% CI: 0.68, 0.72, p < .001) were associated with lower odds of avoidable classification.

The strong age gradients observed in Model 1 raised the question of whether the insurance pattern is uniform across the life course, leading us to examine avoidable ED rates within insurance-by-age subgroups.
Subgroup Patterns by Age
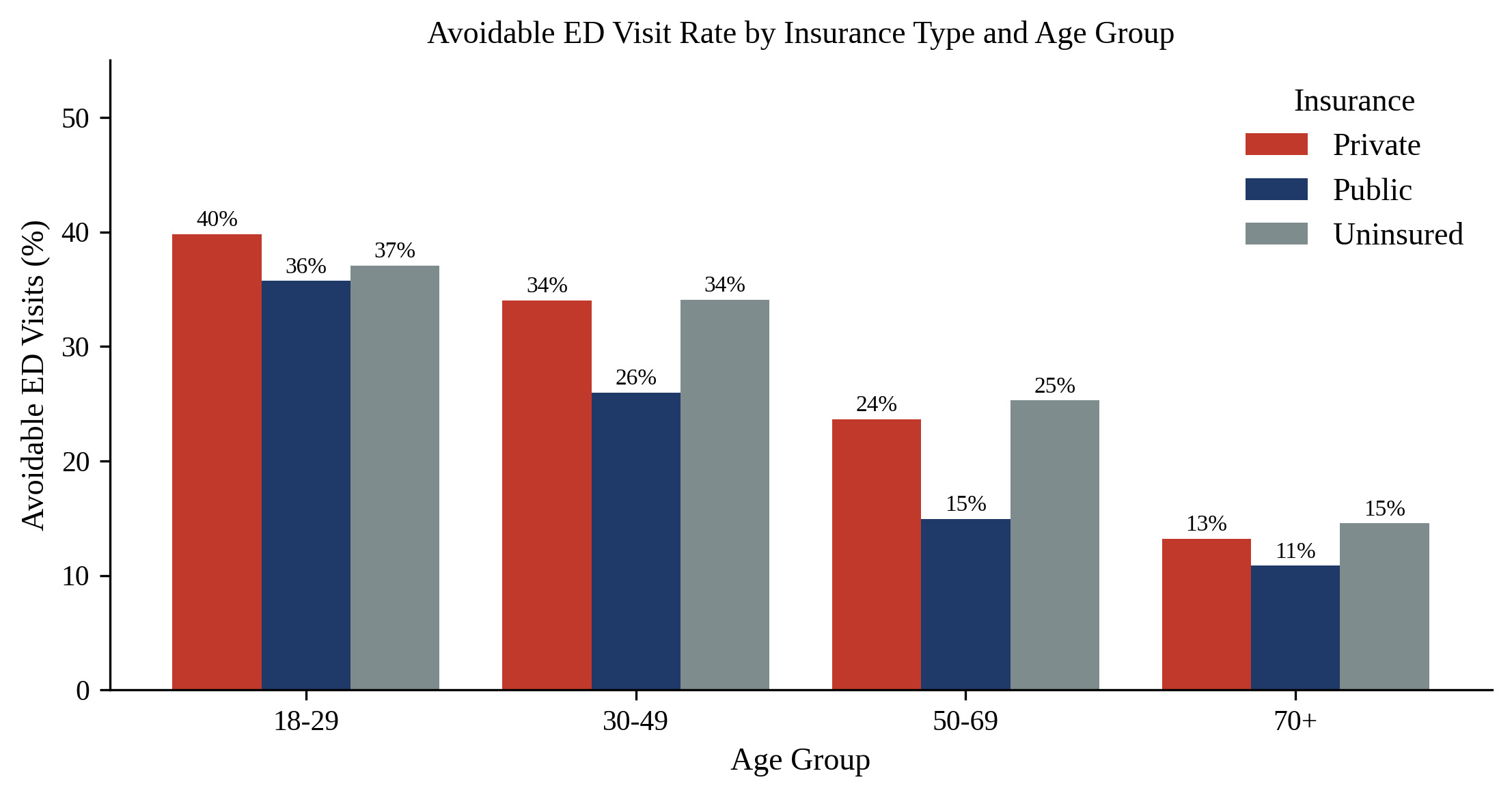
Observed avoidable ED visit rates by insurance type and age group are displayed in Figure 3. Among adults aged 18 to 29, avoidable ED rates exceeded one in three across all insurance groups (40% Private, 36% Public, 37% Uninsured). The gap between privately insured and publicly insured patients widened with age, reaching 9 percentage points in the 50 to 69 group (24% vs 15%) before narrowing among adults age 70 and older (13% vs 11%). Across age strata, uninsured patients tracked closely with privately insured patients in their avoidable ED rates, consistent with the modest adjusted association observed in Model 1. The convergence in the 70-and-older group is consistent with the dual-eligible structural reality that most adults in that group share Medicare coverage and similar clinical complexity regardless of secondary insurance.

Effect Modification by Mental Health Diagnosis
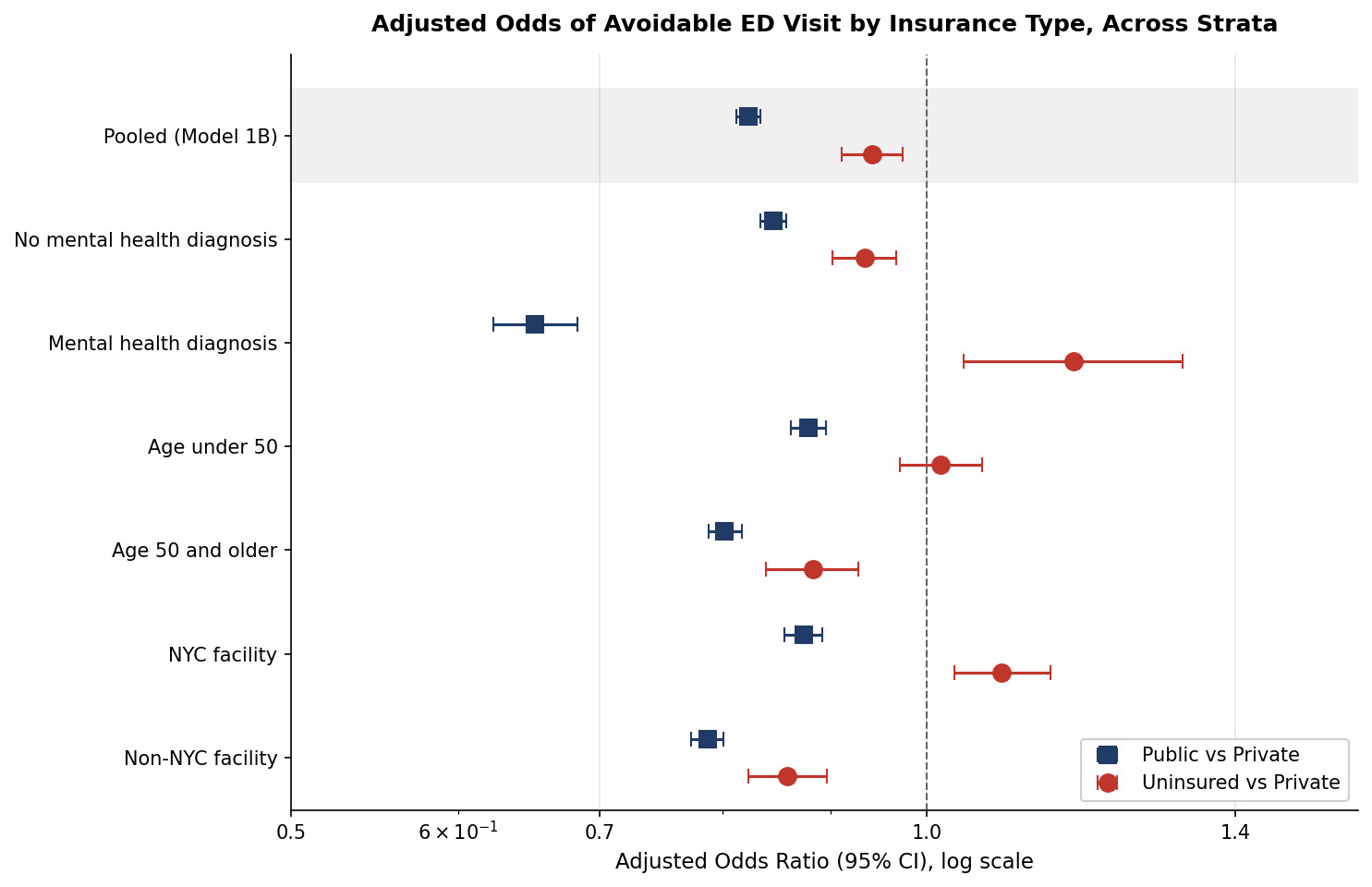
The age-stratified pattern in Figure 3 motivated more systematic examination of effect modification, beginning with mental health diagnosis. The interaction model (Model C) yielded a strongly significant Insurance × Mental Health interaction (likelihood ratio chi-square = 408.15, df = 2, p < .001). Stratified estimates are presented in Table 5 and visualized alongside the geographic and age strata in Figure 4. Among ED visits without a mental health diagnosis (n = 1,202,458), the protective effect of public insurance was modest (AOR = 0.85, 95% CI: 0.83, 0.86, p < .001), and uninsured status was associated with 7% lower adjusted odds (AOR = 0.93, 95% CI: 0.90, 0.97, p < .001), consistent with the pooled estimates. Among visits with a mental health diagnosis (n = 56,397), the public-insurance effect more than doubled in magnitude (AOR = 0.65, 95% CI: 0.62, 0.68, p < .001), while the uninsured association reversed direction and became significantly associated with higher odds of avoidable classification (AOR = 1.17, 95% CI: 1.04, 1.32, p = .009). The magnitude of the interaction is substantial enough that the pooled estimate substantially understates the public-insurance effect among the mental-health subpopulation.
Having documented substantial heterogeneity by mental health diagnosis, we next examined whether the primary findings were robust to alternative specifications of insurance, age, and geography.
Sensitivity Analyses
Results of the four sensitivity analyses are presented in Table 6 and Figure 4. The primary finding (lower adjusted odds of avoidable ED among publicly insured patients) was robust across all specifications, with effect sizes ranging from AOR = 0.79 to 0.88. The uninsured association, however, exhibited substantial heterogeneity. Reclassifying Managed Care, Unspecified payments to Public produced essentially identical estimates (Public AOR = 0.82, 95% CI: 0.81, 0.83). Disaggregating the Uninsured category revealed that the apparent protective effect was driven entirely by the Miscellaneous/Other group (AOR = 0.81, 95% CI: 0.77, 0.85, p < .001), while Self-Pay alone was associated with 8% higher adjusted odds of avoidable classification (AOR = 1.08, 95% CI: 1.03, 1.13, p < .001). Age stratification confirmed that the public-insurance protective effect was stronger among adults 50 and older (AOR = 0.80, 95% CI: 0.79, 0.82) than among adults under 50 (AOR = 0.88, 95% CI: 0.86, 0.90), and that the uninsured association was null in the younger stratum (AOR = 1.02, 95% CI: 0.97, 1.06).
The geographic stratification produced the most striking finding. In Non-NYC facilities, both publicly insured and uninsured patients showed significantly lower adjusted odds of avoidable ED visits than the privately insured (Public AOR = 0.79, 95% CI: 0.77, 0.80; Uninsured AOR = 0.86, 95% CI: 0.82, 0.90; both p < .001). In NYC facilities, however, the uninsured association reversed direction: uninsured patients in NYC had 9% higher adjusted odds of avoidable ED visits than the privately insured (AOR = 1.09, 95% CI: 1.03, 1.14, p = .002), while public insurance remained protective but more modestly so (AOR = 0.87, 95% CI: 0.86, 0.89, p < .001). This NYC versus Non-NYC reversal among uninsured patients is consistent with the known density of NYC safety-net infrastructure (NYC Care, NYC Health + Hospitals) that channels low-acuity uninsured presentations to ED settings where care is reliably accessible regardless of payment status, in contrast to outside NYC where uninsured patients more often defer non-emergent visits.

Model Fit
Model 1 demonstrated good explanatory performance for a logistic model of administrative outcomes. The McFadden pseudo R-squared was 0.31, the log-likelihood was -413,681, and the likelihood ratio test against the null model yielded chi-square = 371,987 (df = 26, p < .001), indicating that the included covariates collectively contributed substantial explanatory power.
Discussion
In a statewide sample of more than 1.25 million ED-related discharges in New York during 2022, privately insured adults had the highest adjusted odds of avoidable ED visits, with publicly insured adults showing 18% lower odds and uninsured adults showing 7% lower odds in fully adjusted models. The pooled findings replicate and extend prior SPARCS-based work that used a multinomial framework with insurance as the outcome,18 confirming that the inverse association between public insurance and avoidable ED utilization in New York is robust to richer clinical adjustment, including diagnostic category, type of admission, and medical/surgical care. The pattern is consistent with two decades of national-survey evidence showing that, after the major payer-specific shifts associated with Medicare and Medicaid coverage, the privately insured population has shown disproportionate growth in primary-care-treatable ED visits.17,34 The pooled estimate, however, conceals substantial heterogeneity. Mental health diagnosis and geographic context substantially modified the insurance-avoidable gradient, with the public-insurance protective effect doubling in magnitude among mental health visits and the uninsured association reversing direction among NYC patients. The remainder of this discussion places these patterns within a structural interpretation that resists framing populations as passive overusers and instead recognizes the strategic logic that often underlies emergency department use.
Interpreted through Andersen’s Behavioral Model of Health Services Use and socio-ecological theory,40–42 these findings suggest that insurance type operates less as a simple marker of coverage and more as a proxy for the configuration of enabling resources and structural constraints within which patients make ED care-seeking decisions. Taken together, these patterns are more consistent with strategic use of the ED under constrained access than with passive “overuse,” particularly among publicly insured and uninsured adults whose options for timely primary and specialty care are structurally limited.
Strategic Use of Emergency Departments by Insurance Type
The substantial attenuation of the public insurance effect from a crude OR of 0.48 to an adjusted OR of 0.82 indicates that age structure and clinical severity account for the bulk, but not all, of the bivariate association. Once age, risk of mortality, length of stay, and diagnostic category are controlled, an independent residual association persists. Read through Andersen’s tripartite framework, the residual association points to differences in enabling factors (insurance benefit design, primary care supply, transportation) and predisposing factors (health beliefs, prior experiences with the health system) rather than to differences in clinically evaluated need.40,41
Privately insured patients may use the ED for low-acuity concerns that are technically appropriate for primary care, reflecting after-hours convenience, employer-sponsored insurance designs that include high deductibles for primary care, or physician availability constraints.4,5,17 Cunningham and May documented two decades ago that growth in ED utilization was concentrated among the insured rather than the uninsured,34 and Pukurdpol and colleagues subsequently showed that primary-care-treatable ED visits had increased disproportionately among publicly insured populations only after baseline coverage equalization, leaving the privately insured as a persistent locus of non-emergent ED use.17 For publicly insured and uninsured patients, the lower observed rates of avoidable ED visits do not reflect lower need; they reflect a different pattern of strategic decisions, including delaying care until acuity escalates, using EDs as the gateway to specialty care or care coordination they cannot otherwise access, and avoiding settings that feel risky to navigate. Both mechanisms can operate simultaneously and produce the same observed gradient, and both are visible in the New York data.
Rural and Urban Primary Care Deserts
The 8% lower adjusted odds of avoidable ED visits among patients receiving care in New York City facilities, relative to the rest of the state, is notable and aligns with the geographic patterning of primary care supply. Though the Patient Protection and Affordable Care Act (ACA) expanded coverage for preventive and primary care visits and required all Marketplace plans to cover emergency services as one of ten essential health benefits,51 it did not guarantee a proportional expansion of primary care providers, and persistent primary care deserts in both rural communities and urban neighborhoods mean that EDs often remain the only consistently available site of care.52–54 Workforce projections indicate continuing physician and nurse shortages,11,12 and Medicaid managed care network adequacy varies dramatically across plans and regions, with documented disruptions to patient-provider continuity that drive patients toward the ED as a default access point.55,56 In primary care deserts (rural counties without sufficient practitioner supply, inner-city neighborhoods with chronic underinvestment, and immigrant-dense neighborhoods with linguistic and structural barriers), the hospital is often the most reliable site of care available. Patients in those settings are not over-using EDs; they are using the only setting that is structurally available, and the avoidable label, applied retrospectively from administrative codes, mischaracterizes a rational response to a fragmented access architecture.30,56,57
Specialty Care and the Referral Bypass Hypothesis
A second strategic logic is the use of EDs to bypass cumbersome specialty referral processes. For patients who require specialty evaluation, the ED can also function as a route around cumbersome outpatient referral systems and narrow networks; in contexts where specialists demand prior authorization, have long wait times, or are absent from local safety-net clinics, presenting through the ED may be one of the few reliable ways to obtain timely diagnostic work-ups and specialty consultation. Patients with conditions that require ongoing specialist input (rheumatology, cardiology, infectious diseases, neurology) face wait times of weeks to months for outpatient specialty appointments in many regions. The ED, by contrast, offers immediate diagnostic workup, on-site consultation, and the possibility of same-day specialty engagement. Studies of urban EDs have demonstrated that they function as a meaningful entry point into specialty care for populations otherwise excluded; for example, Leider and colleagues showed that an urban ED could effectively engage HIV-positive individuals in specialized HIV care from the ED setting itself, bypassing the multi-step community referral pathway.58 Emergency department patient navigators have been shown to successfully connect patients to follow-up care across rapidly evolving health care systems,59 and patient navigator models have been used to build medical homes for multiply diagnosed populations.60 The findings of the present study (higher avoidable ED odds for circulatory and digestive presentations, lower odds for respiratory, infectious, and kidney/urinary presentations) are consistent with a referral-bypass interpretation, in which patients with chronic conditions that map to specialty access (cardiac, gastrointestinal) use the ED as a structurally available entry point.
Chronic Conditions, Disability, and Medical Complexity
Patients with chronic and medically complex conditions face a particularly intricate calculus when deciding where to seek care. These dynamics are particularly salient for people living with chronic and medically complex conditions such as HIV, sickle cell disease, systemic lupus erythematosus, and severe asthma, for whom the ED often represents a predictable node where diagnostic imaging, laboratory work, and specialty input can be coordinated within a single episode of care.61,62 People living with HIV, especially older adults experiencing multimorbidity, increasingly navigate a care landscape characterized by Ryan White HIV/AIDS Program clinics, primary care providers, and specialty co-management.63–65 Sickle cell disease, lupus, severe asthma, and other conditions associated with episodic acute exacerbations frequently require ED-level evaluation that is not avoidable in any meaningful clinical sense, even when the presenting symptom is coded as Minor severity.61,62 The lower adjusted odds of avoidable classification among patients with respiratory and infectious diagnoses in our model is consistent with this clinical reality. People with disabilities, particularly those whose accommodations are not consistently met in outpatient settings, may also default to EDs because EDs are obligated under EMTALA and the Americans with Disabilities Act (ADA) to evaluate and accommodate them, whereas private outpatient practices are often less accessible in practice. Racial disparities in chronic condition outcomes within and across primary care practices further compound these dynamics.61 Reading the avoidable label as overuse in these populations risks pathologizing a medically rational pattern of care-seeking and obscures the structural failures of upstream care.
Older Adults, Dual Eligibles, and Younger Adults
Life-course position structures both the avoidable ED outcome and the policy levers available to address it. Adults aged 70 and older showed the lowest adjusted odds of avoidable ED classification, reflecting their higher clinical complexity, near-universal Medicare coverage, and the protective effect of established care relationships. Among older adults and dual-eligible Medicare-Medicaid beneficiaries, the observed pattern likely reflects a rational strategy to manage multimorbidity, functional limitations, and fragmented coverage across Medicare, Medicaid, and long-term services and supports; the Older Americans Act and CMS Special Needs Plans are designed to address these care-coordination challenges, and coordinated care models that integrate primary, behavioral, and long-term services and supports are associated with reduced avoidable ED use among this population.64,66 At the other end of the life course, adults aged 18 to 29 showed the highest avoidable ED rates across all insurance categories. For youth and younger adults, elevated avoidable ED rates may arise from limited age-appropriate primary care access, high unmet behavioral health needs, and insurance designs (including high deductibles and narrow networks) that make same-day ambulatory care difficult to obtain. Young adults face well-documented challenges in establishing primary care relationships, particularly during transitions from pediatric to adult care, and many remain underinsured or uninsured despite the ACA dependent-coverage expansion.19,23,49 Tailored interventions for emerging adults, such as health navigation programs, transition clinics, and behavioral health integration, are essential complements to the broader system reforms discussed below.15,59,60
Immigration Enforcement, Substance Use, and Structural Avoidance
A subset of patients in New York State actively avoids formal health care settings, including EDs, because of the perceived risk of immigration enforcement, surveillance, or referral to law enforcement. For undocumented and mixed-status families, the ED is embedded in a broader landscape of immigration enforcement and surveillance; reports of immigration enforcement near hospitals and uncertainty about information sharing with immigration authorities can generate structural avoidance, particularly for non-urgent symptoms. Documented and undocumented immigrants face elevated barriers to emergency care across multiple domains, including fear of detention, language access, and lack of coverage, with undocumented immigrants comprising the largest share of the uninsured in New York.30,31,45,67 The escalation of Immigration and Customs Enforcement (ICE) activity in or near health care settings during 2025 has further chilled care-seeking among immigrant communities and complicated the obligations of EDs under EMTALA, the Health Insurance Portability and Accountability Act (HIPAA), and state confidentiality protections.18,68,69 These patients are not simply non-utilizers; they are making constrained, strategic choices to delay or avoid care when they perceive risk of exposure to immigration enforcement, which can subsequently surface as higher-acuity ED presentations. State emergency safety nets respond to these dynamics in narrowly tailored ways: in the District of Columbia, for example, Emergency Medicaid is available only for residents with an emergency medical condition who meet income criteria but are otherwise ineligible for full-scope coverage due to citizenship or immigration status, illustrating how state policy configures a narrow emergency safety net for uninsured and immigration-restricted populations.70
People who use substances similarly face barriers to calling emergency services or presenting to EDs because of fear of arrest or referral to child welfare authorities, despite Good Samaritan laws designed to mitigate these risks.71 Similarly, for patients with substance use disorders, the ED often functions both as an accessible site for acute withdrawal or intoxication and as one of the few settings where linkage to treatment or harm reduction is offered, even when these episodes are coded as avoidable. These structural avoidance dynamics manifest in our data as lower adjusted odds of avoidable ED classification among publicly insured and uninsured patients, but the mechanism is not lower need; it is deferred or foregone care, which can be expected to surface later as higher-acuity inpatient encounters and worse health outcomes.
Insurance Architecture and Cost-Related Care Decisions
The architecture of US insurance products shapes care-seeking in ways that are largely invisible in administrative data but central to the strategic calculus described above. Catastrophic Marketplace plans, which combine low monthly premiums with deductibles approaching $8,700 in recent years, are designed to protect against very high costs but leave enrollees exposed to substantial out-of-pocket spending for routine ambulatory care, even as they must cover emergency services as an essential health benefit.51,72,73 Many privately insured patients also carry supplemental hospital indemnity plans that provide lump-sum cash benefits for hospital admission or ICU stays, effectively subsidizing ED and inpatient episodes while leaving outpatient and specialty costs comparatively less buffered.74 Short-term limited-duration plans, where permitted, often exclude preexisting conditions, offer limited benefits, and may not be available at all in jurisdictions such as the District of Columbia, where regulators have prohibited their sale; this variation illustrates how state policy configures the emergency safety net for medically complex and uninsured patients.75 At the same time, federal protections against surprise billing for emergency care limit out-of-network cost exposure for ED encounters, including some air ambulance services, while comparable protections for scheduled outpatient visits remain more fragmented, making the ED in some cases a more financially predictable site of care.76 For uninsured patients, EMTALA establishes the obligation to screen and stabilize regardless of ability to pay,68 and Emergency Medicaid covers acute episodes for some otherwise-ineligible residents.70
An additional, underexamined financial mechanism shaping ED decision-making is the proliferation of medical credit cards and related financing products marketed at the point of care. These cards frequently advertise zero-interest promotional periods but rely on deferred-interest structures and high annual percentage rates, such that any unpaid balance at the end of the promotional window triggers retroactive interest on the original charge amount. Regulators and advocates have documented that patients often are not fully informed of these terms, encounter high-pressure marketing in emergency and outpatient settings, and incur substantial interest costs, particularly when large medical balances prove difficult to pay off quickly.44,77 Although the present administrative data cannot observe uptake of these products, their spread underscores that patients presenting to the ED, especially those uninsured or underinsured, are navigating not only clinical risk but also a landscape of predatory financial instruments that may influence when and where they seek care. The point is not that any single product drives ED use; the point is that the patient is making a sophisticated, financially constrained decision, and the avoidable label flattens that complexity.
Diagnostic and Severity Coding Mechanics
Diagnostic category effects in Model 1 illuminate the mechanics of severity coding. Circulatory and digestive diagnoses were more likely than the Other category to be classified as Minor severity, consistent with high-volume conditions such as chest pain, atypical cardiac presentations, gastritis, and gastroenteritis that are frequently evaluated and discharged from the ED without requiring inpatient escalation. Infectious diseases, respiratory conditions, and kidney and urinary conditions were less likely to be classified as Minor, reflecting the higher acuity profile of admissions in those categories. The very large effect of non-minor risk of mortality (AOR = 0.05) and the smaller but consistent effects for length of stay and care type indicate that the avoidable ED outcome, as operationalized through APR Severity, is largely a function of the same clinical signals that drive admission and resource intensity, an important caveat for any policy interpretation that conflates Minor severity with primary-care-treatable status.1,35–37
Mental Health Heterogeneity in the Insurance-Avoidable Gradient
The most consequential finding of this analysis is the strong effect modification by mental health diagnosis. The pooled estimate (Public AOR = 0.82) and the no-mental-health-stratum estimate (Public AOR = 0.85) substantially understate the protective effect of public insurance among visits with a mental health diagnosis (Public AOR = 0.65). The uninsured association exhibits an even more striking pattern, reversing direction from a marginally protective association in the no-mental-health stratum (AOR = 0.93) to a significantly elevated association among mental health visits (AOR = 1.17). The likelihood ratio test (chi-square = 408.15, p < .001) confirms that this heterogeneity is unlikely to reflect chance, and the magnitude of the interaction has both clinical and policy significance.
The most plausible interpretation involves selective access to outpatient behavioral health care. Publicly insured patients seeking care for mental health concerns may be more likely to access psychiatric care through structured Medicaid behavioral health benefits, integrated managed care plans, certified community mental health programs, and the broader safety-net infrastructure of New York City and the state, reducing the likelihood that their eventual ED presentation is for a low-acuity concern.78 Privately insured patients may experience narrower behavioral health networks relative to their medical networks, sometimes referred to as the mental health parity gap, and may be more likely to present to the ED for non-emergent concerns that fall outside contracted outpatient access. Uninsured patients are heterogeneous in their access pathways: NYC supports the NYC Care program and a robust public hospital system that expand ambulatory access for uninsured residents, while Non-NYC settings rely more heavily on hospital safety-net care.47,79 The strong protective effect of public insurance among mental health visits should be read partly as evidence that publicly insured patients with mental health concerns are admitted at higher acuity, consistent with deferred or delayed access to outpatient psychiatric care.78,80
It is also important to note a measurement caveat: the APR Severity of Illness scale was originally developed for medical-surgical encounters and tends to assign Minor severity to many psychiatric encounters that are clinically high-acuity from a behavioral health standpoint. As a result, the proportion of mental health visits classified as avoidable in our data likely overstates the extent to which these visits could realistically have been managed in ambulatory settings. The directional pattern of the interaction is robust to this caveat, but the absolute levels should be interpreted with the limitations of severity coding for psychiatric presentations in mind.78,80
Geographic Heterogeneity: NYC Versus Non-NYC
The geographic stratum reversal among uninsured patients is the second major heterogeneity finding. In Non-NYC facilities, uninsured status was associated with 14% lower adjusted odds of avoidable ED visits (AOR = 0.86), consistent with the deferred-care interpretation that has dominated the safety-net literature. In NYC facilities, the same comparison yielded 9% higher adjusted odds (AOR = 1.09), a directional reversal that the pooled estimate masks. This finding is consistent with the structural reality of NYC’s safety-net infrastructure, which is among the densest in the United States. NYC Health + Hospitals operates 11 acute-care hospitals and a network of community-based clinics, NYC Care expands ambulatory access for uninsured residents,79 and the borough-level distribution of EDs is geographically more accessible to uninsured residents than is the case in many upstate counties.47,79 Uninsured patients in NYC may use the ED for low-acuity concerns because EDs are reliably available, EMTALA guarantees evaluation regardless of payment, and the No Surprises Act limits balance-billing exposure for emergency care.44,68 Outside NYC, the calculus shifts: uninsured patients in upstate counties face longer distances to hospitals, less dense safety-net infrastructure, and greater financial exposure, leading to deferral of non-emergent visits. This geographic heterogeneity has direct policy implications, particularly for safety-net infrastructure investment in counties without comparable density.28,53,54,57
Sensitivity and Robustness
The sensitivity analyses establish two important boundary conditions on the primary findings. First, the Self-Pay versus Misc/Other disaggregation reveals that the apparent protective effect among uninsured patients is driven entirely by the Miscellaneous/Other category (AOR = 0.81), while Self-Pay alone is associated with 8% higher adjusted odds of avoidable classification (AOR = 1.08). The Miscellaneous/Other category likely includes patients whose payment was administratively complex (charity care, pending Medicaid applications, internationally insured) and whose clinical and demographic profile may differ systematically from Self-Pay patients. The Self-Pay finding aligns with the NYC stratum result and supports a coherent interpretation: when uninsured patients have meaningful access to EDs (NYC density, safety-net care, EMTALA-protected evaluation), they use them for low-acuity concerns at rates similar to or higher than the privately insured. Second, the age stratification confirms that the public-insurance protective effect is stronger in older adults (AOR = 0.80) than in younger adults (AOR = 0.88), consistent with the dominant role of Medicare in the older stratum, where coordinated geriatric care across primary, specialty, and post-acute settings reduces the likelihood that ED presentations are for low-acuity concerns.64,66 Together, these sensitivity findings reinforce the structural-strategic interpretation: care-seeking patterns reflect the constellation of available alternatives, not insurance type per se.
Strengths and Limitations
Strengths of this analysis include the use of a large, all-payer statewide sample, the inclusion of richer clinical adjustment than has been applied in prior SPARCS-based avoidable ED analyses, and the use of binary logistic regression with avoidable ED as the explicit outcome, which is more directly aligned with the policy question of interest than prior multinomial frameworks. Limitations include the cross-sectional nature of SPARCS, which precludes causal inference and individual-level longitudinal analysis. The avoidable ED definition relies on the APR Severity of Illness classification, which captures clinical acuity at evaluation but does not perfectly map to the conceptual definition of an avoidable visit; ambulatory-care-sensitive condition algorithms such as the New York University ED algorithm35,36 and machine-learning approaches37 would offer complementary specification but require diagnostic-code-level inputs not consistently coded in this de-identified file. The dataset reflects inpatient-flagged encounters with an ED indicator, so the findings may not generalize to ED visits that did not result in admission or that occurred in non-hospital urgent care settings.38 Race and ethnicity are derived from administrative records and are subject to misclassification. Comorbidity adjustment using validated indices such as the AHRQ Elixhauser measure39 was not feasible with the available variables. Pandemic-related shifts in ED utilization are also relevant to the 2022 analytic year, as avoidable ED rates and care-seeking patterns evolved substantially during and after the COVID-19 surge.81 The Uninsured category includes Self-pay, Miscellaneous, and Other payment typologies and may be heterogeneous in ways the data do not allow us to disaggregate. Finally, residual confounding by unmeasured factors such as primary care availability, transportation,31 housing stability, and immigration status is likely.
Implications for Policy and Practice
These findings argue against framing avoidable ED utilization as a problem driven principally by public insurance enrollees in New York. We organize implications across three actor groups (hospitals, payers and policymakers, and federal statutory frameworks), recognizing that the most consequential interventions cut across all three.
Hospitals and Health Systems
Hospitals can implement ED-based patient navigator programs that connect non-emergent presentations to longitudinal primary, behavioral, and specialty care, with documented success in rapidly evolving care environments.59,60,82 Embedding community health workers in ED workflows extends this reach into populations that face linguistic, immigration-related, or substance-use-related barriers to formal care.82 Hospital-based safety-net programs such as NYC Care, with documented success in connecting uninsured residents to primary care,47 should be expanded and replicated. ED operational reforms (improved triage, reduced left-without-being-seen rates,13 optimized patient flow,9 ambulance diversion mitigation,8 and integration with after-hours urgent care79) address the throughput consequences of avoidable visits without misattributing them to patient behavior.
Payers and Policymakers
Payers can reduce financial barriers to primary care for the privately insured population that drives avoidable ED rates in this analysis, including elimination of cost-sharing for primary care visits and expansion of telehealth as a first-contact alternative. Medicaid managed care plans should prioritize network adequacy and continuity of physician relationships, given evidence that disruptions in patient-provider continuity drive ED utilization.55,56 State and federal policymakers should sustain Medicaid expansion and address gaps in coverage for immigrants and other populations excluded from the ACA, recognizing that uninsurance is itself a structural driver of avoidable hospitalization.19–22,45,67
Federal Statutory Frameworks
Several federal frameworks already provide partial scaffolding for the structural changes implied by these findings. The Emergency Medical Treatment and Labor Act (EMTALA) establishes the universal obligation to screen and stabilize emergency presentations regardless of payer, but does not address the upstream access architecture that channels avoidable visits to EDs in the first place.68 The ACA expanded coverage and primary care benefits but did not generate proportionate increases in primary care provider supply, particularly in rural and inner-city primary care deserts.16,20,52,53 The Americans with Disabilities Act (ADA) requires accommodations across health care settings, but enforcement has been uneven in outpatient practices, contributing to default ED use among patients with disabilities. The Ryan White HIV/AIDS Treatment Extension Act provides a high-functioning model of payer-of-last-resort care for an entire chronic disease population, with documented impact on housing stability and clinical outcomes among people with HIV63–65; comparable infrastructure for other chronic conditions could substantially reduce avoidable ED visits among medically complex patients. The Older Americans Act and complementary CMS dual-eligible programs provide coordination scaffolding for older adults but require sustained funding and integration with primary care to deliver on that promise. Healthy People 2030 articulates the social determinants framework within which all of these mechanisms must operate.15 The combined message is that avoidable ED utilization is not a behavior problem amenable to demand-side discipline; it is a system design problem that requires coordinated action across statutes, payers, and care delivery models.
Future Research
Future research should examine mental health and substance use diagnoses as modifiers of these patterns, given the public health significance of behavioral-health-related ED utilization and the limitations of the severity-of-illness proxy for these encounters.71,78,80 Continued surveillance with future SPARCS releases and complementary all-payer claims analyses will be valuable to characterize whether these patterns shift as Medicaid redetermination, post-pandemic care-seeking, immigration enforcement dynamics, and urgent-care expansion evolve in New York State.79,81 Mediation analyses examining the pathways through which insurance type translates into avoidable ED classification (via primary care continuity, specialty referral, transportation, and immigration concerns) would clarify which structural levers are most actionable. Qualitative work centering the voices of patients in primary care deserts, immigrant communities, and chronically ill populations would complement administrative-data findings with the strategic logic that this analysis can only infer.
Conclusion
In a 2022 statewide sample of more than 1.25 million ED-related discharges in New York, privately insured adults had the highest adjusted odds of avoidable ED visits, while publicly insured and uninsured patients had lower odds even after accounting for demographic, geographic, and rich clinical adjustment. The relationship was strongly modified by mental health diagnosis (with the public-insurance protective effect more than doubling among mental-health visits and the uninsured association reversing direction) and by geographic area (with uninsured patients in NYC showing the opposite pattern from those outside NYC). The directional finding from prior SPARCS-based work18 is robust and replicates with binary logistic specification, and the new heterogeneity findings clarify that the pooled estimate conceals dynamics with direct policy relevance. These patterns push against assumptions of public insurance overuse and reframe avoidable ED utilization as a structurally patterned, often strategic response to fragmented primary care, specialty referral barriers, mental health parity gaps, immigration enforcement, and the geographically uneven distribution of safety-net infrastructure. Policy and health system strategies should engage all insurance groups, address the mental health parity gap among privately insured patients, sustain investment in safety-net infrastructure outside NYC, and leverage existing federal frameworks (EMTALA, ACA, ADA, Ryan White HIV/AIDS Treatment Extension Act, Older Americans Act) to address the underlying access architecture, treating patients as strategic actors navigating a constrained system rather than as passive overusers of one they did not design.
Acknowledgments
The primary author would like to extend heartfelt thanks to Dr. Circe Le Compte for her invaluable mentorship, guidance, and encouragement throughout the research process. This research was conducted as part of the Boston Congress of Public Health Research Scholars Program (BCPH-RSP), which supports student-led scholarship in health equity and social justice. The author also expresses gratitude to the BCPH-RSP faculty for their support and commitment to fostering impactful public health research.
Disclosure Statement
This study involved secondary analysis of de-identified, publicly available data from the New York State Statewide Planning and Research Cooperative System (SPARCS) Hospital Inpatient Discharges 2022 file, released by the New York State Department of Health through Health Data NY.¹ The dataset contains no protected health information as defined under the Health Insurance Portability and Accountability Act (HIPAA) and is freely available without application or data use agreement. Because the analysis used only publicly available, fully de-identified data, this study did not constitute human subjects research under 45 CFR 46.102 and was therefore exempt from Institutional Review Board review under 45 CFR 46.104(d)(4)(ii), which provides exemption for secondary research involving the use of identifiable private information that is publicly available. No IRB protocol number was assigned.
Individual Author Biographies
Nickol Georgy is an undergraduate student at the University of Southern California majoring in Quantitative Biology and minoring in Applications of Artificial Intelligence. She is an aspiring researcher who is passionate about advancing health equity through community-based work, policy reform, and interdisciplinary research, and is particularly interested in research that bridges social justice with medicine and policy.
Dr. Circe Gray Le Compte (she/her/hers) is Co-CEO of the Boston Congress of Public Health (BCPH), a 501(c)(3) nonprofit dedicated to democratizing public health through the lens of social justice, where she also serves as Chief Technology Officer, Director of BCPH Studio. She has served as editor-in-chief or co-editor-in-chief of the Boston Congress of Public Health Review (BCPHR, formerly the Harvard Public Health Review/HPHR Journal) since 2015, joining the journal’s founding board as Deputy Editor in 2014. In addition, she has worked in leadership positions at several national HIV nonprofits and health communication organizations.
Dr. Le Compte holds Master of Science and Doctor of Science degrees from Harvard University, Harvard T.H. Chan School of Public Health, where she concentrated in social and behavioral sciences theory and research methods and in racial and sexual/gender minority health. Her research has explored novel interventions, such as soap operas and PhotoVoice, to improve health outcomes among medically underserved populations. Her doctoral dissertation used qualitative and quantitative methods to examine how lived experience shapes the conceptualization of health and sexual harm-reduction practices among Black/African-American gay and bisexual men and transwomen.