INTRODUCTION
As of 2023, the international burden of chronic kidney disease (CKD) has been estimated to be 788 million people aged 20 years and older, with CKD being the ninth leading cause of death globally, and the 12th leading cause of Disability Adjusted Life Years (DALYs).1 In the context of a global CKD prevalence of 14.2%, the prevalence of CKD in African Americans in the United States is 18.4% while that of Sub-Saharan Africans ranges from 2-41%.2 The clinical determination of chronic kidney disease is based upon two variables: glomerular filtration rate (GFR) that could be either measured or calculated and albuminuria which is a measurable parameter.3 CKD is characterized by a calculated GFR less than 60 mL/min/1.73 m2 over the course of 3 months or a urine albumin to creatinine ratio greater than 30mg/g. Given that acquiring the gold standard measurable parameters is both costly and time-consuming, calculated or estimated GFR (eGFR) that utilizes biomarkers such as creatinine and Cystatin C is the most commonly used method of kidney function analysis. Directly correlated to patient muscle mass, creatinine represents a less stringent biomarker of renal function as compared to its newly recognized Cystatin C counterpart. Yet, at least 50 different equations including the Cockcroft and Gault as well as the Modification of Diet in Renal Disease (MDRD) equations are based on the creatinine marker since initial presentation in literature in 1957.4
Developed in the United States in 2009, the Chronic Kidney Disease Epidemiology (CKD-EPI) equation includes age, sex, and race factors and is the former standard recommended by Kidney Disease: Improving Global Outcomes (KDIGO) international guidelines. The race factor is incorporated in this version of the equation as it accounts for the differentially higher creatinine levels demonstrated by African American individuals as compared to Caucasian counterparts in observational studies measuring GFR. Movements toward removal of the racial factor from the original CKD-EPI formula launched in 2019 with discussions of the social construction of race and ultimately culminated in the race-free CKD-EPI 2021 equation.5 Though race as a social construct has been weaponized to create subdivisions used to subject whole groups to grossly aversive discrimination, the race factor of the CKD-EPI equation accounts for biological differences in inherent glomerular filtration rates observed in population studies. Prior to the introduction of the race factor in 2009, decreased accuracy as compared to measured GFR was broadly noted particularly in Black Americans. Elimination of this race factor now introduces disparities in medication access as seen in an observational retrospective study looking at metformin access among patients with CKD.6 In this particular study, transition to the race blind CKD-EPI equation translates into disqualified eligibility for a low cost diabetes disease modifying medication. Since other disease modifying therapies for hypertension and heart failure such as RAAS modulators and SGLT2 drugs also have GFR limiting criteria, a move to a race naive CKD-EPI equation may also limit access to these life changing medications.
Nevertheless, since its entry into the literature, the National Kidney Foundation-American Society of Nephrology Task Force has recommended the 2021 CKD-EPI equation for implementation in clinical laboratories (Table 1).7 As of 2023, 65.8% of US laboratories reported adoption of the 2021 CKD-EPI equation.8 Barriers to adoption of this equation in Europe include reluctance to shift from the current European Kidney Function Consortium (EKFC) standard that itself does not include a racial factor and that has demonstrated consistent accuracy in European populations.9 In Sub-Saharan Africa, a population study in Malawi, Uganda, and South Africa demonstrated a 14 point lowering of median eGFR with the 2021 equation, and has therefore stalled overall implementation of the updated equation.10 In Asia, the reclassification of a greater proportion of its population to lower risk GFR categories begs further investigation before complete adoption of the 2021 CKD-EPI equation on a continental level.11 The Canadian Society of Nephrology, however, has commissioned a committee to mediate the adoption of the newer equation in agreement with the National Kidney Foundation-American Society of Nephrology Task Force.
Despite median eGFR of up to 4mL/min/1.73m2 lower and higher values compared to gold standard measured GFR (mGFR) for Black and non-Black individuals respectively, the 2021 race free equation is currently the silver standard for diagnosing kidney disease across the KDIGO CKD classification brackets.13 With omission of race in this later equation, Black individuals are projected to have 2.0% higher prevalence of CKD while non-Black persons have 1.5% lower prevalence compared to previous race adjusted formulae.13 This reclassification of Black individuals into higher stages of CKD has negative implications leading to contraindication and dose restriction for certain prescription drugs, unwarranted referral for nephrology care and kidney transplantation, and decreased eligibility for kidney donation and clinical trial participation. Though the 2021 CKD-EPI equation’s tendency to underestimate eGFR in Black populations and to overestimate eGFR in non-Black counterparts has been noted, the equation continues to dictate treatment protocols and referrals for kidney replacement therapies on an individual basis. With more Black individuals being classified into higher risk CKD stages within the context of the 2021 CKD-EPI equation, more of this population may be pre-emptively condemned to dialysis, a thrice weekly therapy that comes with high economic and quality of life costs.
A narrative review targeting health care providers is therefore undertaken to analyze the extent of the effect of the 2009 and 2021 iterations of the CKD-EPI equations on measures of renal function in Black populations across the globe. The objective of this review is to assess the eGFR outputs for the two equations across various cohorts in an effort to quantify the effect of the elimination of the race factor on CKD classification, eGFR accuracy, and drug eligibility. This review aims to shed light on the downstream effects of an already implemented health care policy change in eGFR calculation. It targets providers who must use these calculations to refer patients to nephrology specialists who then must use eGFR along with other measures to determine dialysis necessity.
METHODS
The following narrative review is conducted in accordance with an ‘a priori’ protocol published in Open Science Framework.14
Search strategy
An initial limited search of PubMed is undertaken to identify articles on the topic. The text words contained in the titles and abstracts of relevant articles are then used to develop a full search strategy in conjunction with a librarian. The reference lists of all included sources of evidence are screened for additional studies. The databases searched include Embase, Web of Science, and PubMed. Studies published in English only and published between 2021 and 2024 are included in the final review.
Inclusion criteria
The review seeks to include studies from across the globe that look at both male and female adults aged 18 and above. Analytical as well as descriptive observational studies including prospective and retrospective cohort studies, case-control studies and analytical cross-sectional studies are considered for inclusion. Research article types such as conference abstracts and research letters are excluded during the screening process. Studies where only non-Black populations are analyzed are excluded from the review. Only studies that directly compare the CKD-EPI 2021 equation with the CKD-EPI 2009 race adjusted equation head to head are included. Only studies with outcomes in median GFR, mean GFR, percent accuracy, CKD reclassification, medication administration, medication dosing, and treatment access are included in the narrative review.
Source of evidence selection
Following the search, all identified citations are collated and uploaded into Covidence software and duplicates are auto-removed. Titles and abstracts are then screened for alignment with the inclusion criteria. Potentially relevant sources are retrieved in full and their citation details recorded. Reasons for exclusion of sources of evidence at full text that do not meet the inclusion criteria are also recorded and reported in the narrative review. The results of the search and the study inclusion process are reported in full and are presented in a PRISMA flow diagram.15
Data extraction
Data are extracted from papers included in the review using a word-based data extraction tool developed by the reviewer. The data extracted include specific details about the participants, concept, context, study methods, and key findings relevant to the review question such as citation details, country of study, total participants, and population kidney disease status. One of the primary outcomes includes accuracy or the proportion of patients with eGFR values within a given threshold of measured GFR, whether that be within 15% of mGFR (P15) or 30% of mGFR (P30). Quality assessment of the included studies is conducted using the Critical Appraisal Skills Program Checklist for Descriptive/Cross-Sectional Studies.16 Graphical representation of extracted data through forest plot and bar graph is conducted via R statistical programing software version 4.2.3.
RESULTS
Identification of publications for Data Extraction
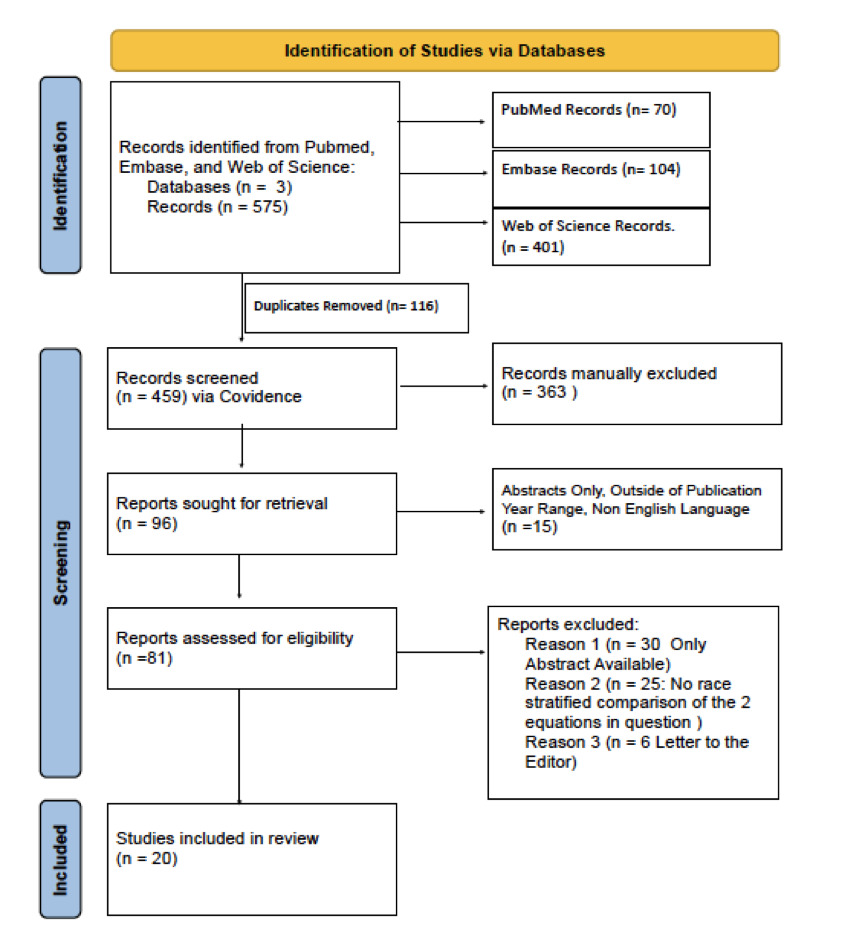
Following use of defined MeSH terms, 575 publications are identified via the 3 disclosed databases. This is then narrowed to 459 publications upon computerized removal of duplicate records (Figure 1). Using Covidence to then screen these records allows for the exclusion of 363 records based on unfitting populations of study, for example, those looking at ‘eGFR’ as it pertains to ‘epidermal growth factor receptors’. Comparisons between GFR equations not of interest are also grounds for exclusion during this screening phase. Of the remaining 96 records, 15 are excluded based on pre-established inclusion criteria, leaving 81 reports assessed for review inclusion. After eliminating publications that do not assess race stratified comparisons of the 2009 and 2021 CKD-EPI formulae via median GFR, mean GFR, CKD reclassification, and drug eligibility, a total of 20 full text articles are included in the review.12,17–35

Outcomes measured to compare CKD-EPI equation performance
The 20 articles included in the review all report on the percentage of the study populations represented by Black individuals, with people identifying as Black representing from 2.5% to 100% (n = 45- 24,898,373) of populations under study (Table 2). The majority of these publications capture CKD-EPI performance through mean GFR, with 14 out of 20 (70%) studies measuring this outcome as shown in Table 3. 10 out of 20 (50%) articles measure CKD reclassification as the outcome variable, all concluding that the 2021 CKD-EPI equation comparatively worsens CKD stage in Black individuals (Table 2). 4 of the 20 (20%) studies evaluate the effect of the differential eGFR calculations on drug eligibility, concluding that the race naive 2021 equation disqualifies from 1.0% to 25% more Black individuals from drug consideration criteria compared to the 2009 race considerate equation (Appendix II). 3 (15%) of the articles compare the two equations to measured GFR and report outcomes within 15% or 30% from these measured values bi-directionally. 4 studies (20%) report median GFR, demonstrating 14 point greater GFR for the 2009 CKD-EPI equation in a cohort in Kenya and 6-7 point greater GFR in 2 US cohorts undergoing nephrectomy (Appendix II).
Comparison of eGFR calculations in Black populations
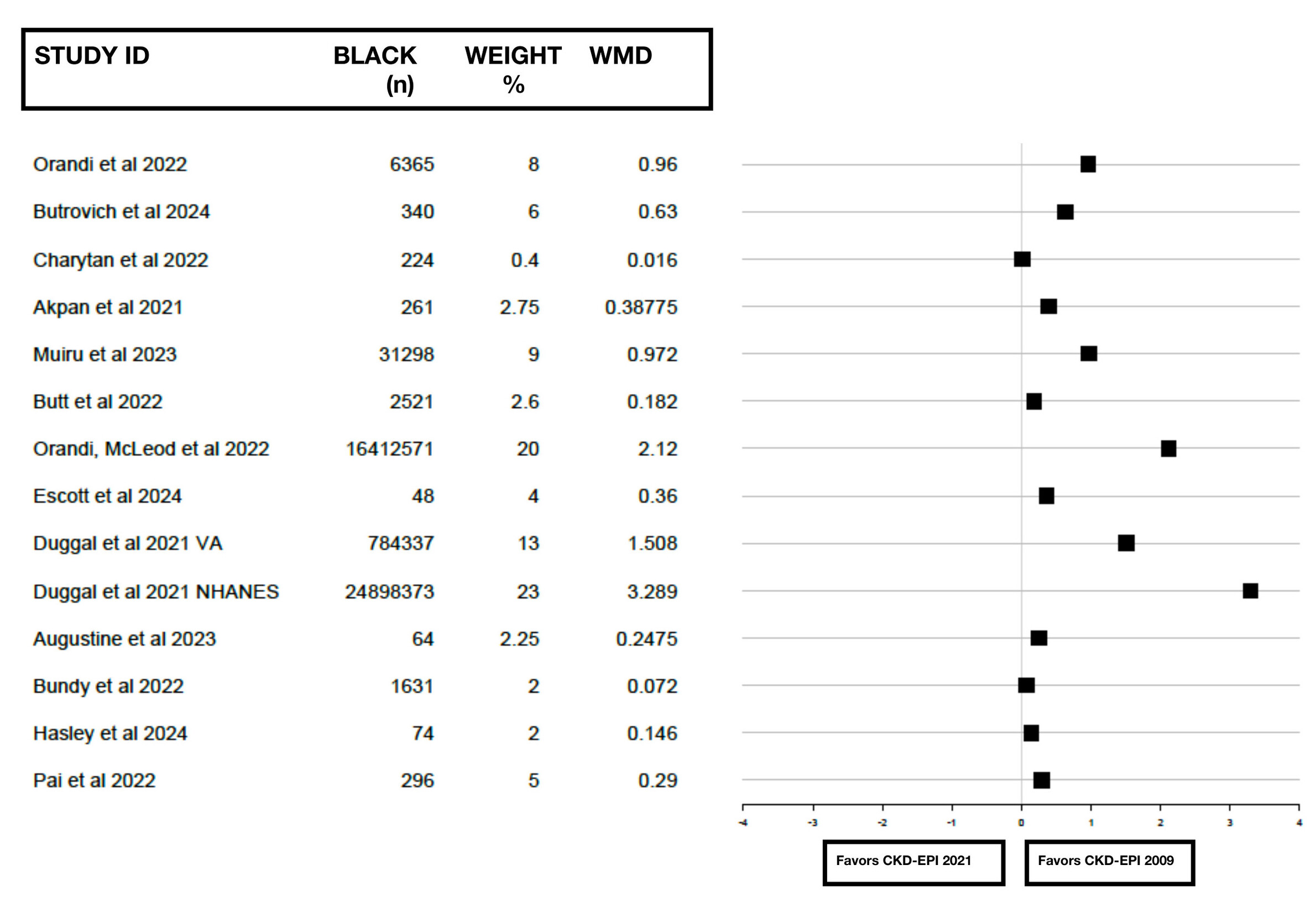
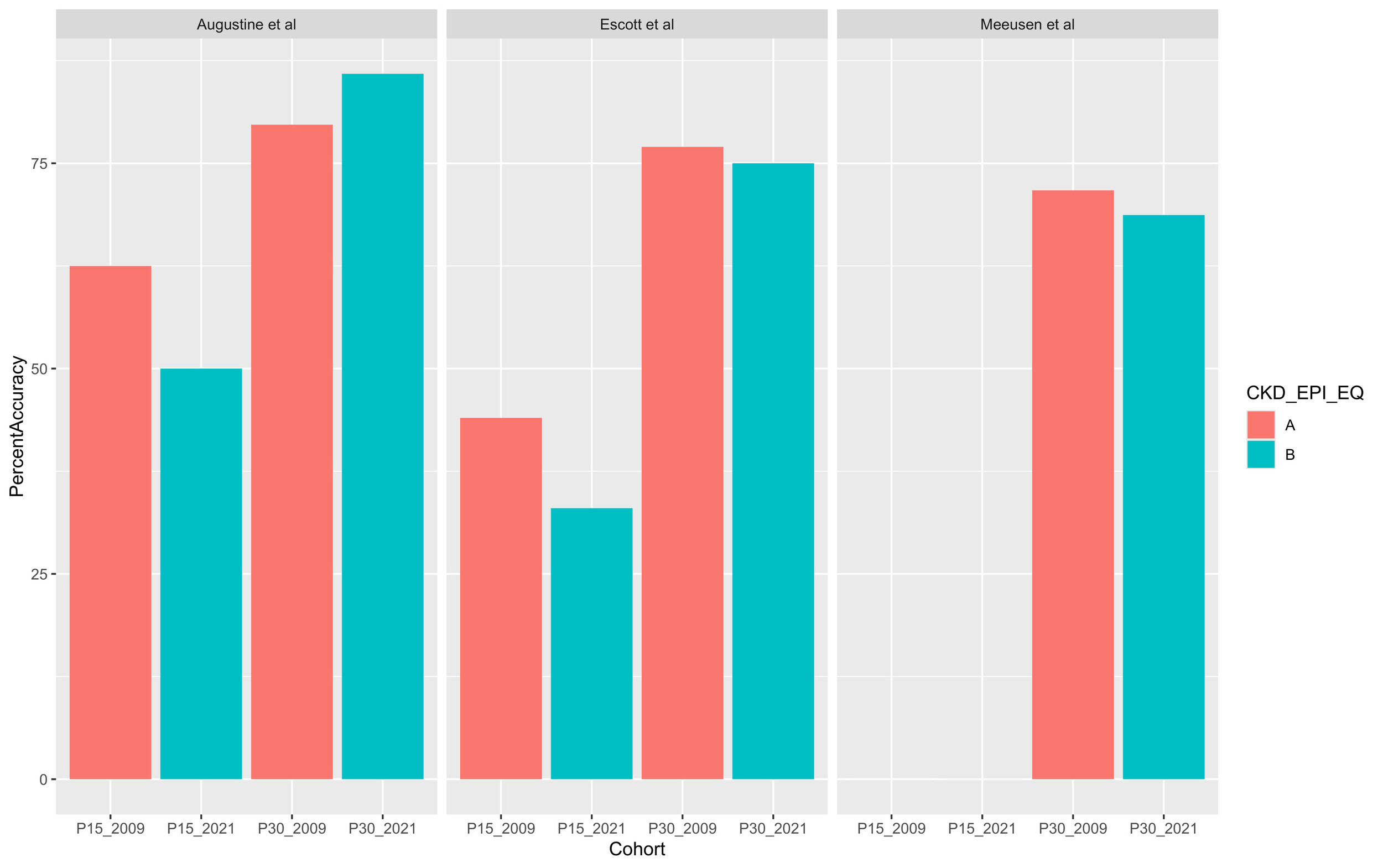
Mean eGFR reported across the 14 studies measuring this outcome in populations ranging from 48 to 24,898,373 (n) Black individuals is 89.757 (18.65, SD standard deviation) using the 2009 race inclusive equation compared to 80.357 (17.32) using the 2021 equation (Table 3). The difference between the mean eGFR outcomes favors the CKD-EPI 2009 equation in all 14 cases, with mean difference ranging from +4 to +14.3 points. Greater eGFR values are consistently seen with the 2009 equation even when weights are assigned to each study based on both the number of Black persons (n) represented by the study as well as the health status of the cohort individuals (Figure 2). When comparing the 15 percent accuracy outcome, the 2009 CKD-EPI equation demonstrates 11-12.5% greater accuracy than the 2021 equation in two cohorts (Figure 3). The CKD-EPI 2009 equation again demonstrates greater accuracy than the 2021 equation with margins between 2-3% in 2 of the 3 cohorts analyzing 30 percent accuracy, alluding to the concept that the Black race modifier of the 2009 equation lends to estimated filtration rates closer to the gold standard measured GFR.
_between_egfr_calculated_by_the_2.jpg)
_and_p30_(egfr_within_30__.jpg)
DISCUSSION
Obesity, diabetes, and hypertension are the leading risk factors for chronic kidney disease development. African Americans have higher prevalence of these three comorbidities compared to their White counterparts with 76.4% compared to 68.5% prevalence of obesity, 18% compared to 9.6% prevalence of diabetes, and 43.3% compared to 29.1% prevalence of hypertension respectively.36 Contributing to the increased burden of CKD in the Black population is poverty with 20% of African Americans in the United States falling below the federal poverty line compared to 9% of Caucasians in 2018. Lacking health literacy and insurance further yields to the nearly 3 fold increased incidence of end stage renal disease (ESRD) in the Black minority population compared to White counterparts and to the 1.5 fold increased incidence compared to the general population. Given the immense healthcare usage costs, time expense, and physical demands that CKD and ESRD impose on the individual, it is crucial that diagnosis is accurate, timely, and not premature.
Before implementation of the race naive 2021 eGFR creatinine-based equation, bias in eGFR calculations in Black and non-Black individuals was noted, with increased values and therefore healthier CKD classifications observed in non-Black populations of appropriately matched creatinine levels.13 It is unclear, however, whether this bias towards lower eGFR values in Black persons represent true worsened renal function masked by the 2009 equation or exaggerated CKD staging that then leaves this population with unwarranted replacement therapy referrals and limited access to renally dosed medications. Muiru et al. present findings comparing the risk of CKD progression for black individuals with the 2009 and 2021 eGFR equations, demonstrating 3 fold risk of progressing from CKD 3 to CKD stage 4 or 5 (HR 3.06, 2.60 -3.62 CI) compared to non-Black counterparts using the 2009 equation as opposed to about 2 fold risk (HR 1.71, 1.45- 2.02 CI) of the same disease progression with the 2021 race naive calculations.14 While the lower risk of progression between these particular CKD stages observed with the 2021 formula implies that accelerated rates of kidney disease progression at later CKD stages may have been masked by the 2009 black race modifier, Muiru et al. looks at HIV/AIDS cohorts as opposed to the healthy subjects that formed the basis of the original 2009 CKD-EPI equation.
A case report of a 72 year old African American woman further discusses the differential kidney disease progression rates in CKD stages 4-5 represented by the two equations.37 This case describes a woman who qualifies for renal transplant referral based on the race unadjusted equation who ultimately waits 1 year to be added to the transplant list because the race modified equation categorizes her with an eGFR higher than the threshold for transplant referral. If the equation without race modifier had been applied to her case, she would have been referred for renal transplant 12 months earlier. An alternative interpretation of this particular case report is to view the patient’s lacking need of dialysis for 12 months as proof of concept that the 2009 CKD-EPI accurately depicts disease extent and reflects the urgent rather than emergent need for renal replacement therapy.
Earlier iterations of the equations estimating kidney function were derived exclusively from studies involving Caucasians and only considered this racial group. It turns out that these equations had decreased accuracy in Black Americans leading to the introduction of race based modifiers statistically derived from diverse populations. Inclusion of the 1.159 Black race correction factor in the original CKD-EPI equation of 2009 increases eGFR by 15.9% to account for the higher serum creatinine and differential tubular secretion seen in this population at counterpart-matched mGFR, age, and sex.20,32 The mean serum creatinine levels observed in non-Hispanic Black men based on the Third National Health and Nutrition Examination Survey of 1988-1994 was 1.25 mg/dL compared to a mean of 1.16 mg/dL observed in Caucasian males.38 Estimated GFR values based on observed elevated levels of serum creatinine markers were calibrated against measured clearances such that mean creatinine values of the respective racial groups were made equivalent and the biological differences in creatinine filtration were accounted for in the 2009 CKD-EPI formula.7,39 The 2009 eGFR formula therefore accounts for the phenotypic differences observed between Black individuals and their non-Black counterparts in NHANES III-IV through the 1.159 Black race correction coefficient.
The K correction factors for sex, 0.70 mg/dL for females and 0.90 mg/dL for males, present in both the race conscious and race naive creatinine based equations are in fact the mean serum creatinine levels specifically observed in healthy Caucasian populations in NHANES IV.7,40,41 The 2021 race naive creatinine based eGFR formula, therefore, inadvertently carries forward remnants of racial bias by including the K correction factor that is itself imbedded in observed racial differences in serum creatinine levels. Though the implementation of the 2021 race naive eGFR equation is aimed at eliminating race as a construct from an equation estimating a biological phenomenon, its incorporation of the K factor defeats the purpose of this public health policy change. By reverting to a version of the equation that only studied kidney function in White populations, the policy change ignores the inherent differences across ethnicities and unintentionally reinforces a racial bias of its own. It is in this clinical context that race is indeed a phenotypic factor and not a social construct as referred to in recent global discussions.
The idea of race as a social construct in reference to the eGFR formulae likely did not surface until a more precise serum marker of renal clearance, Cystatin C, entered the arena and demonstrated reduced racial bias.42 The 2012 CKD-EPI Cystatin C equation is represented in Table 1. Bias, defined as mGFR – eGFR, is closest to zero with the 2012 CKD-EPI cystatin C equation in Black and non-black individuals as compared to not only the 2009 and 2021 creatinine based eGFR equations but also the 2021 CKD-EPI creatinine/cystatin C combined formula with K correction factor. Additionally, within a meta-analysis encompassing 44,721 participants, cystatin-C based equations not incorporating the K correction factor demonstrated no significant difference in P30 accuracy between Black and non-black individuals with P30 of 85.3% and 85.7% in Black and non-Black persons respectively.42 This means that with cystatin C based equations even without a race factor, both Black and non-Black persons are designated to CKD classifications that accurately define their long term kidney health status and that grant them equitable access to renally dosed medications. As opposed to race naive creatinine based eGFR equations, race naive cystatin C based equations such as the 2012 CKD-EPI cystatin C allows for patients to access medication and treatment modalities including dialysis when medically indicated. Unlike the creatinine/cystatin C combined formula, Cystatin C based calculations without the K correction factor have the potential to remove structural barriers to renal replacement therapies among not only Black individuals but also other ethnicities who require this step up in treatment.
CONCLUSION
The presented narrative review yielding 20 studies published following National Kidney Foundation Task Force guideline recommendations in 2021 provides further evidence towards the increased eGFR and percent accuracy demonstrated by the 2009 race inclusive creatinine-based equation in Black individuals. Findings allude to the idea that renal function estimated based on creatinine markers should include the Black race modifying coefficient considering the physiological and not the social nature of increased serum creatinine levels measured in this particular population. While the use of the 2021 race unadjusted equation has a goal of eliminating racial bias from kidney function calculations, inclusion of the K factor perpetuates observations based solely on a Caucasian population. Use of race adjusted creatinine based eGFR or Cystatin C based eGFR calculations therefore leads to less biased representations of kidney function in Black individuals, which leads to less misdiagnosis of CKD, less preclusion from therapeutic considerations, and less premature referral for renal replacement dialysis. Perhaps the race naive 2021 CKD-EPI equation would truly become race naive and would furthermore depict less underestimation of eGFR in Black populations if it were to disregard the racially biased K correction factor. If not for the cost of Cystatin C assessments, race naive Cystatin C eGFR calculations would offer the most accurate and socially conscious equation to be implemented into national and global policy.
LIMITATIONS
Limitations of this narrative review include the lack of eGFR stratification by age related comorbidities such as diabetes, hypertension, and heart disease as well as the absence of age adjusted definitions of CKD. This review is also limited by the use of creatinine-based GFR formulae instead of Cystatin C based equations, which yield less biased estimations of kidney function. This review does not assess for subgroup ethnic differences within the global Black population and considers these persons of the African diaspora as a single homogenous group. Furthermore, this review does not pursue sub-group analysis by patient setting. As this is a narrative review, this study does not assess publication bias via funnel plot or Egger’s regression test.
FUNDING
No funding sources were allocated for this narrative review.
CONFLICTS OF INTEREST
There is no reportable conflict of interest for this narrative review.
ACKNOWLEDGMENTS
I would like to express sincere gratitude to librarian Janice Lester at North Shore University Hospital for her work towards refining this study’s database search strategy.