Background
Avoidable emergency department (ED) visits, in which patients seek non-emergency services that do not require diagnostic or screening services, procedures, or medications in the ED rather than primary care settings, place considerable stress on hospitals.1,2, ED visits overall have increased in recent years,1 with one study reporting over 140 million ED visits in the United States in 2021 alone, resulting in a rate of 43 visits per 100 people.2 A significant number of these ED visits in the United States fall into the “avoidable” category. A 2017 study of medical records in the National Hospital Ambulatory Medical Care Survey found that approximately 5% (20 million) of the 424 million ED visits among adults aged 18-64 in the United States between 2007 and 2011 were for non-emergent reasons.3 Since the pandemic, an estimated 24% of adults4 have used the ED for non-emergent issues, most notably for mental health and dental conditions that the ED is not equipped to treat.5 Urban centers like New York City have even higher avoidable ED rates. Recent literature indicates a continuation of ED overuse in New York City, with 40% of ED visits classified as avoidable in 2024.6
As such, avoidable ED visits represent a pressing and often overlooked public health issue in the United States. Overcrowding in EDs7 strains on hospital infrastructure, drains financial resources5 and contributes to workforce burnout.8 Health care workforce studies note an increasing number of nurses leaving the profession,9 while a nationwide shortage of physicians is expected by 2030.10 In addition, the longer life spans of most populations in the United States have contributed to chronic conditions expected to increase overall demand on healthcare systems, further intensifying pressure on emergency services.11 Among patients, avoidable ED visits create long wait times,12 contributing to increased morbidity and mortality for time-sensitive conditions, such as stroke and acute myocardial infarction,13 and overall poorer health outcomes14,15 and increased mortality.15 All clients, including those in need of emergency care, are more likely to leave ED waiting rooms before accessing treatment, which contributes to the chances of early death from treatable emergency conditions.12
Many of these avoidable ED visits may be associated with patients’ insurance types, which in the United States primarily fall into three categories: private, public, and uninsured.16 Private insurance refers to health coverage provided through employer-sponsored plans (in which the employer pays part of the cost and the employee pays the remainder), individually purchased plans, and other group plans obtained through nongovernmental organizations, such as unions and associations.
Public insurance refers to coverage paid for or supplemented by government structures for United States citizens, including coverage purchased through Patient Protection and Affordable Care Act (ACA) programs. It also includes Medicare, which covers health care for persons aged 65 and older and younger people with permanent disabilities, and Medicaid, a joint federal and state program that supports eligible low-income persons in the United States.17 While initially limited to low-income pregnant women and children, passage of the ACA enabled states to allow coverage for all low-income persons.18 At the time of this writing, 41 states (including New York) and Washington, D.C. have opted to expand Medicaid to their residents.19
Millions of people in the United States are uninsured due to factors such as residence in a state that has not participated in Medicaid expansion, immigration status, or limited health literacy, resulting in poorer health outcomes.20 Being underinsured or uninsured can limit access to preventive and primary care, resulting in a dependence on EDs for often deferred primary care concerns and ultimately increased hospitalizations and overall costs.16,21
In this study, we examined the association between insurance type and avoidable ED visits in the State of New York. We hypothesized that ED visits would be associated with insurance type, with most avoidable ED visits in NYC occurring among individuals with public coverage or who are uninsured, due to the increased challenges these individuals face in accessing primary care compared to those with private insurance.22
Methods
We used data from Health Data New York, a data bank maintained by the New York State Department of Health.23 We specifically used the publicly available dataset, “Hospital Inpatient Discharges (SPARCS De-Identified): 2022,” which contains details on patient characteristics, diagnoses, and charges for the year 2022 and was last updated on April 1, 2025. This file is de-identified and from the Statewide Planning and Research Cooperative System (SPARCS), an all-payer data reporting system, designed to collect discharge information from hospitals.23 The Office of Health Services Quality and Analytics Center for Applied Research and Evaluation provided the data dictionary for this dataset. The data is protected health information and contains discharge details for patients, including diagnoses, treatments, services, and charges. The dataset contains 33 variables, including data from across New York districts and information on ethnicities and age ranges. Our predictor was insurance type, categorized into three groups: Public, Private, and Uninsured. The primary predictor was “severity of illness,” categorized as minor and non-minor, and served as a proxy for avoidable ED and non-avoidable ED visits, respectively.
Avoidable ED visits were operationalized by severity of illness: visits classified as “minor” were considered potentially avoidable, whereas those classified as moderate, major, or extreme were considered non-avoidable. Severity of illness reflects the acuity of the presenting condition at the time of evaluation. Our covariates included demographic variables (Age, gender, race, and Hispanic ethnicity), clinical variables (risk of mortality and length of stay), and geographic variables (facility/care location). (Table 4 provides a detailed variable list.) Race and ethnicity variables were derived from hospital-reported administrative records contained in the SPARCS dataset. Consistent with data collection practices used in statewide hospital discharge systems, race and Hispanic ethnicity were captured as separate variables; however, the de-identified nature of the dataset limited the ability to reliably identify individuals who simultaneously identified as Hispanic ethnicity and White or Black/African American race. Race was categorized as White, Black/African American, and Other Race, while Hispanic ethnicity was treated as a distinct categorical variable. As a result, Hispanic patients were analyzed as a separate group, acknowledging that this category may include individuals who also identify with racial groups represented elsewhere in the analysis.
All analyses were conducted using IBM SPSS Statistics (Version 31.0),24 calculating bivariate (unadjusted) tests between insurance type and all covariates. Correlations among predictors were examined using cross-tabulations, chi-square tests, and Cramer’s V for categorical variables, and Pearson correlations for continuous variables. We then calculated multinomial logistic regressions, which yielded adjusted odds ratios (AORs) and 95% confidence intervals for each Insurance Type category relative to the reference category (private insurance). Model fit was assessed using Likelihood ratio tests, pseudo R-squared statistics (Cox & Snell, Nagelkerke, McFadden), and −2 Log Likelihood values. Cox & Snell, Nagelkerke, and McFadden indices were all calculated to assess model performance. The Nagerlkerke pseudo R-squared was used for reporting and interpretation in the text and figures due to its standardized scaling and interpretability in multinomial logistic regression models.
Results
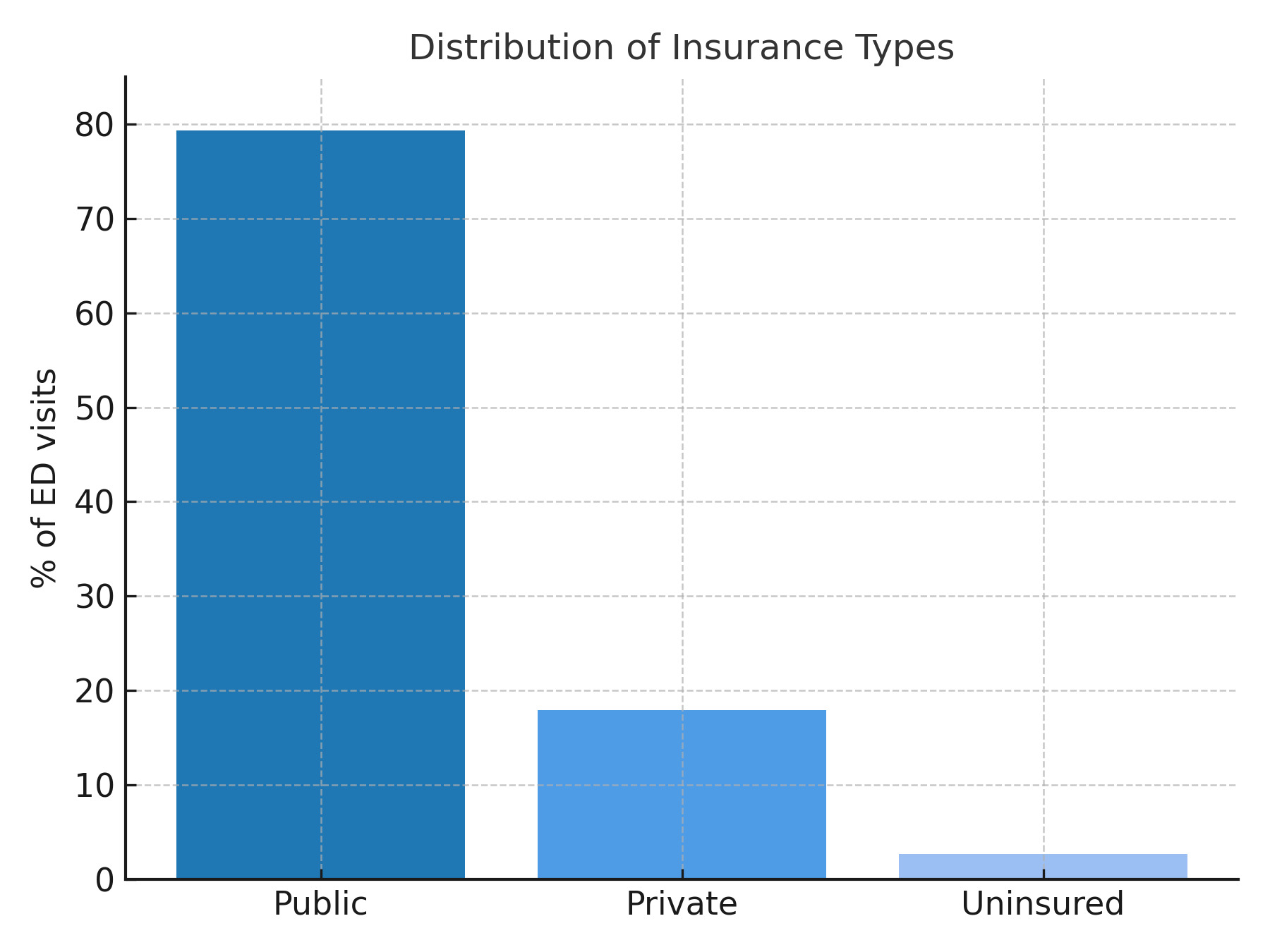
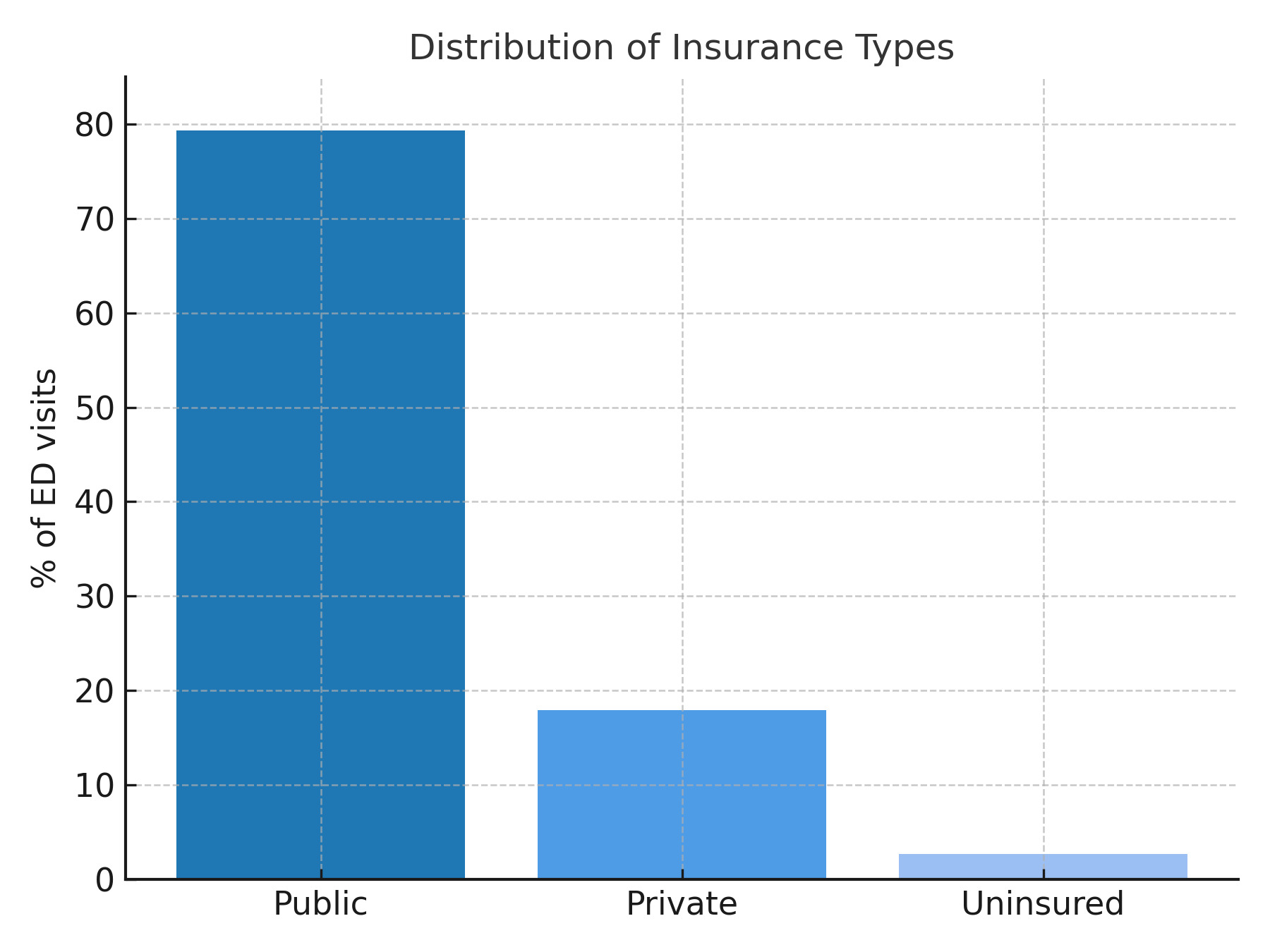
As shown in Table 1, our analytic sample included 430,772 hospital discharges in New York. Most patients were covered by public insurance (72.2%), were female (54.7%), and resided in New York City (67.1%). The sample was racially and ethnically diverse: 53.4% of patients identified as White, 18.3% as Black/African American, and 27% as another race. Additionally, 15.5% identified as Hispanic, 72.8% as not Hispanic, and 11.4% had unknown ethnicity. Most patients were younger than 50 years (42.4%), indicating a relatively young, racially diverse, and predominantly urban population (Table 1). Clinically, most hospitalizations were non-minor in severity (70.2%) and lasted more than 1 day (82.1%), reflecting moderate to severe inpatient encounters. Likelihood ratio tests demonstrated that all predictors significantly improved model fit (p<0.001), as shown in Table 2. Age group, ethnicity, and race exerted the largest effects on insurance classification, indicating strong demographic structuring of payer status. Clinical and geographic variables were also significant, though to a lesser extent.
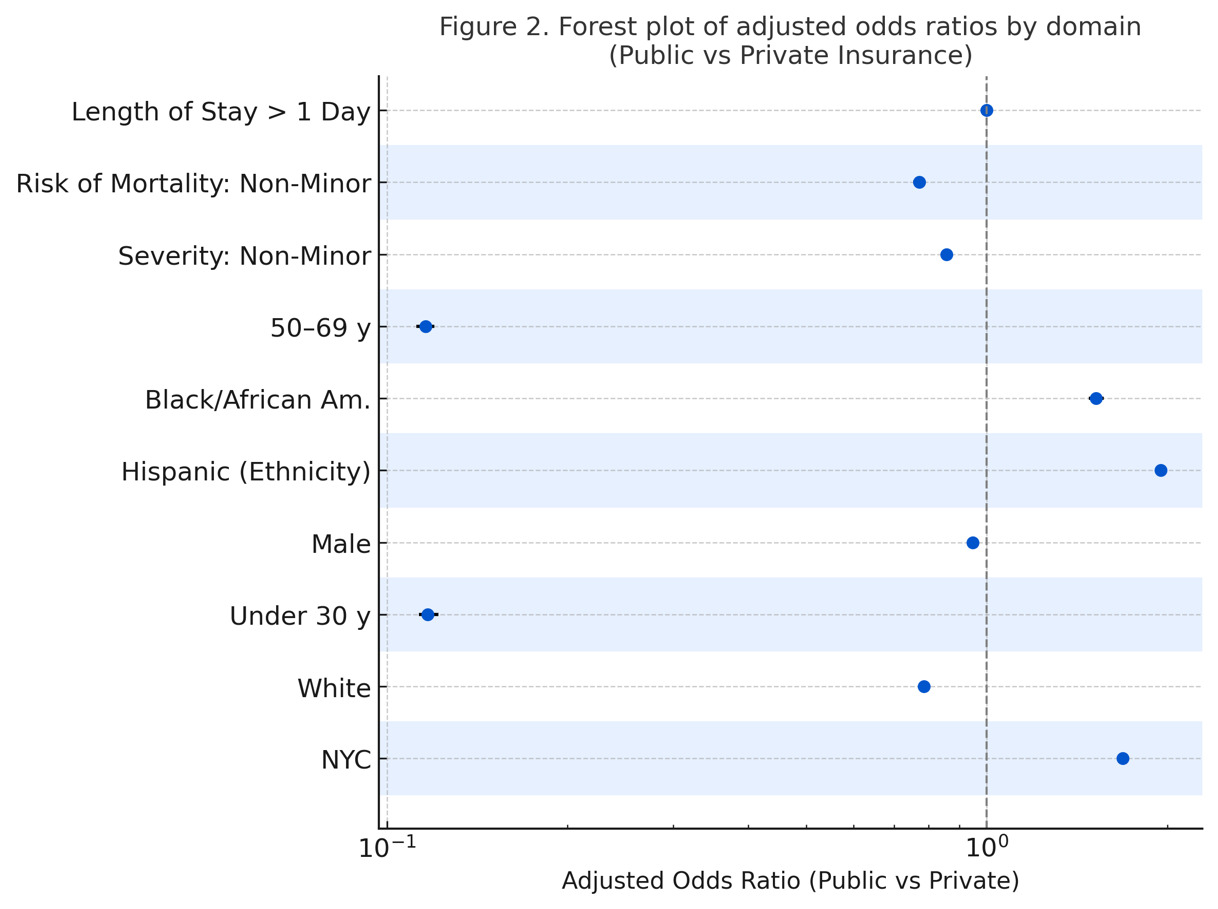
Fully adjusted multinomial logistic regression models (Table 3) identified several demographic, clinical, and geographic characteristics associated with insurance type. Compared with privately insured patients, individuals covered by public insurance were more likely to be older (AORs ≈ 0.12 for both under 30 and 50–69 years), be residents of New York City (AOR = 1.69, 95% CI: 1.66–1.72), Hispanic patients (AOR = 1.95, 1.92–1.98), or Black/African American (AOR = 1.52, 1.48–1.56). Uninsured persons were more likely to be younger, male, non-White, and clinically higher-risk patients.
Racial and ethnic disparities in insurance coverage were substantial (Figure 2). Hispanic patients had nearly twice the odds of having public insurance compared with White patients (AOR, 1.95; 95% CI, 1.82-2.08; p<.001), and Black or African American patients also had higher odds of public insurance (AOR > 1.5; p<.001). These findings highlight persistent inequities in access to private coverage. Geographically, residence in New York City was associated with higher odds of public insurance (AOR, 1.69; 95% CI, 1.60-1.78; p<.001), whereas New York State patients outside of New York City were more likely to have private insurance, suggesting spatial variation in coverage linked to socioeconomic context (Figure 2).
.png)
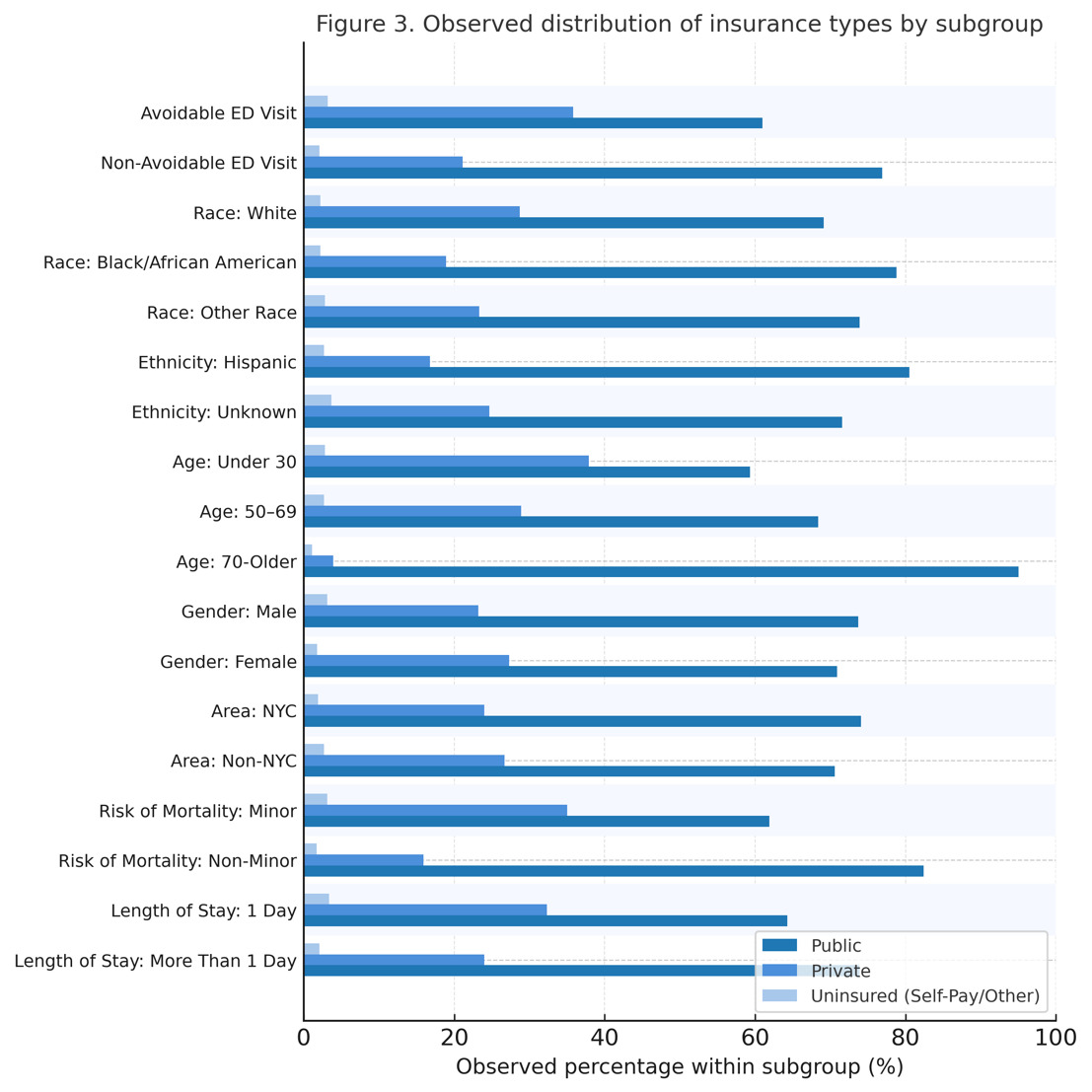
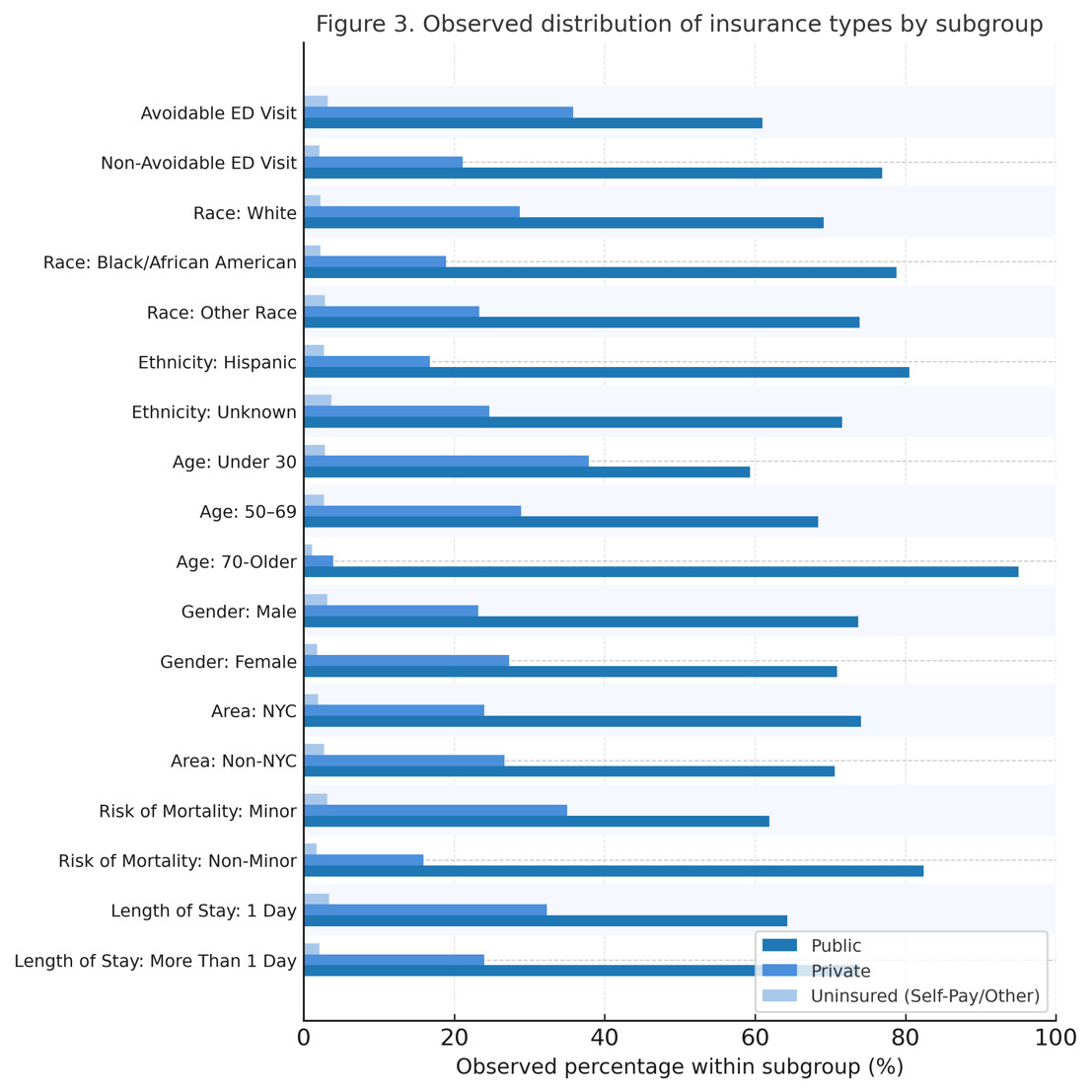
Hospitalizations classified as avoidable ED visits were less likely to be associated with public insurance coverage compared to private insurance (AOR range, 0.77-0.86, all p<0.001) (Figure 3). Consistent with this pattern, publicly insured patients had 14% lower odds of avoidable ED visits than privately insured patients (AOR = 0.86; 95% CI: 0.84–0.87; p<.001). Uninsured patients classified as miscellaneous or other were also significantly less likely than those who are privately insured to engage in an avoidable ED visit (AOR = 0.88; 95% CI: 0.81–0.95; p<.001). Although approximately 30% of encounters were classified as avoidable based on minor severity of illness, a substantial proportion of patients exhibited a higher risk of mortality or longer lengths of stay. Collectively, these findings suggest that public insurance holders and uninsured patients may defer care until there is an emergency or they can no longer defer issues normally addressable through preventive and primary care.
Discussion
Our study found that insurance type was associated with avoidable ED visits in New York, consistent with prior studies.25–28 However, our initial hypothesis that public health insurance holders would make up the majority of avoidable ED visits, as supported in the literature, did not hold true.29–32 Our findings indicated that publicly insured and uninsured patients actually were less likely to engage in avoidable ED visits compared to private insured patients (AOR = 0.86; 95% CI: 0.84–0.87; p<.001). This result challenges commonly held assumptions regarding “Medicaid overuse” of emergency services and highlights the need to reassess how avoidable ED utilization is conceptualized across insurance groups.
These results may, in part, be linked to the passage of the Affordable Care Act (ACA) in 2009, which expanded Medicaid eligibility to all adults who qualified in states that opted for expansion, as well as to additional primary and preventive care services. Before the ACA, patients frequently visited the ED due to limited access to insurance and consistent care, resulting in long wait times and often subpar health care.25 Providers believed that passage of the ACA would result in decreases in ED visits overall,33 as seen in studies that reported a decrease in avoidable ED visits in Medicaid-expansion states compared to non-Medicaid-expansion states,33 as well as a slight reduction in ED use among young adults compared to their older counterparts.34
A 2017 study, however, found that ED visits increased by 2.5 visits per 1,000 people in Medicaid-expansion states after 2014 because of the private insurance options provided by the ACA; patients no longer needed to defer care, but could seek assistance as needed.35,36 For those with public insurance, however, ED use may have decreased due to increases in primary care use. Indeed, coordinated, continuous care reduces reliance on the ED, and is positively associated with improved health outcomes25 with the potential to save $60 billion annually.37 Creating continuity of care, however, cannot be achieved solely through insurance; both private and public insurance holders require support in overcoming barriers to access.33 Indeed, those who turn to the ED for non-emergent issues often view emergency departments as easily accessible, central locations for clinical and behavioral services; primary care clinics and practices may be more challenging to access, particularly in low socioeconomic areas with difficult-to-navigate built environments and limited public transportation.38–42
These factors are evidenced in our analyses (Figure 3). Figure 3 illustrates the distribution of insurance types within categories of clinical severity, length of stay, and mortality risk, rather than direct comparisons of emergency department utilization rates between insurance groups. Across these domains, public insurance holders make up a larger proportion of both avoidable and non-avoidable ED encounters, reflecting their overall predominance in the sample. However, the adjusted regression analyses demonstrate that relative to publicly insured and uninsured patients, privately insured patients have higher odds of presenting with lower-acuity, non-emergent encounters characterized by minor severity, lower mortality risk, and shorter lengths of stay.
Importantly, classifying ED visits as “non-emergent” warrants careful interpretation. Encounters involving mental health, behavioral health, or dental conditions were labeled as non-emergent because emergency departments are not optimally equipped to provide definitive diagnostic evaluation or longitudinal management for these specialized conditions and treatment plans.
Past studies have indicated that historically marginalized persons (such as racial and ethnic minorities, undocumented persons) are more likely to defer emergency and primary care addressable care, experience long wait times, and leave EDs before being seen.12,43 Indeed, recent scholarship suggests that the ACA has encouraged greater primary care use among public insurance enrollees. However, in low-income urban areas, these patients may strategically use the ED when fewer primary care providers and appointments are available.26
Most uninsured persons in the State of New York are likely to be persons who have fallen out of care or are undocumented.27 Though residents of NYC are eligible for programs like NYC Care, which provides uninsured persons in New York City access to low- and no-cost services,28–30 they often defer care until absolutely necessary.28 Substance users and unstably housed persons, for example, often fear being reported to the police.31 Undocumented immigrants, who make up the largest proportion of the uninsured population in New York, as well as documented immigrants seeking asylum may avoid EDs due to fear of detention or questioning by the United States Immigration and Customs Enforcement (ICE)32,44 More broadly, prior research has shown that marginalized and unstably housed populations often avoid formal health care settings due to institutional mistrust and fear of surveillance, which any contribute to delayed or foregone care.45 These concerns have escalated throughout 2025, which saw ICE granted additional powers to enter health care facilities, including EDs, disrupting services, undermining Health Insurance Portability and Accountability Act (HIPAA) protections, and traumatizing patients and staff alike.46 As we write this article, new uncertainties have emerged on how the passage of the Big Beautiful Bill of 2025, which substantially cut Medicaid and Medicare services, will impact avoidable and non-avoidable ED among private and public insurance holders, and those who are uninsured.47
Strengths and Limitations
Our study benefited from access to a large, state dataset with a diverse patient population. However, the cross-sectional design of our study limits causal inference, and residual confounding may be driven by unmeasured factors related to individual clients’ experiences with primary care providers and access, as well as their current lived experiences (housing status, other social needs). Our findings additionally may not be generalizable beyond New York State or to non-hospital settings.
In the State of New York, the association between insurance type and avoidable ED use is nuanced, with privately insured patients demonstrating relatively higher odds of avoidable ED visits than publicly insured and uninsured patients. Our findings push against traditional “Medicaid overuse” narratives among the publicly insured. Rather, they highlight the need for novel approaches to mitigating avoidable ED use, such as improved patient flow and the delivery of safety-net services, and the establishment of enhanced care coordination, after-hours access, and telehealth in primary care. Staff may benefit from additional support and training in working with underserved populations with varying insurance access. Private and public health insurance holders, particularly in “primary care deserts” in low-income urban and rural areas, would benefit from enhanced health care navigation to mitigate unnecessary ED use. Our findings can also inform state and hospital-level policies to alleviate ED crowding and improve equitable access to ambulatory care.
Additional research is needed to explore the mediating pathways between insurance type and avoidable ED use, including clinical and behavioral health factors, length of hospital stay, and risk of mortality. Analyses stratified by age, race/ethnicity, and geographic location would provide insights into the subgroups most in need of interventions and the types of support they require. Qualitative studies featuring focus groups and interviews with patients and providers could further illuminate how insurance benefits, health care practices, and lived experiences shape decisions about ED engagement.
Acknowledgments
The primary author would like to extend heartfelt thanks to Dr. Circe Le Compte for her invaluable mentorship, guidance, and encouragement throughout the research process. This research was conducted as part of the Boston Congress of Public Health Research Scholars Program (BCPH-RSP), which supports student-led scholarship in health equity and social justice. The author also expresses gratitude to the BCPH-RSP faculty for their support and commitment to fostering impactful public health research.
Disclosure Statement
The author(s) have no relevant financial disclosures or conflicts of interest.
About the Author(s)
Nickol Georgy is an undergraduate student at the University of Southern California majoring in Quantitative Biology and minoring in Applications of Artificial Intelligence. She is an aspiring researcher who is passionate about advancing health equity through community-based work, policy reform, and interdisciplinary research, and is particularly interested in research that bridges social justice with medicine and policy.
Dr. Circe Gray Le Compte: She was part of the board that re-founded Boston Congress of Public Health Review, when it was at Harvard University, in 2013. She has served as its editor-in-chief/co-editor-in-chief since 2014. In addition to this role, she serves as co-CEO, CTO, and BCPH Studio lead for the Boston Congress of Public Health, which publishes the journal. She holds Master of Science and Doctor of Science degrees from Harvard University, in social and behavioral sciences, and has decades of communications experience, serving as Director of Communications for the National Minority AIDS Council (NMAC); Senior Director at Impact Marketing + Communications; and Senior Contractor and Senior Director of Health Services Research and Communications with HealthHIV. She holds a postdoctoral fellowship with the Division of Gender, Sexuality, and Health at Columbia University/New York State Psychiatric Institute and works as a senior director of Impact Marketing + Communications.