INTRODUCTION
The number of US states considering legalization of medical and recreational cannabis continues to increase. Since the legalization of recreational cannabis in Colorado and Washington in 2012, additional states followed their pursuits. As of June 2024, recreational cannabis legalization for adults 21 years and older has been passed in 24 states and the District of Columbia.1 This in turn led to more questions on the growing burden of cannabis use, the most commonly used federally illicit drug in the United States.
The 2020 data from the National Survey on Drug Use and Health (NSDUH) revealed that 13% of people aged 12 or older (36.4 million people) in the United States used cannabis in the past month. Almost 6% (1.5 million) are adolescents aged 12 to 17.2 These adolescents may be adversely affected by the well-documented potential short- and long-term adverse effects of cannabis use. These include impaired short-term memory, decreased concentration and problem-solving which affects learning, and alterations in motor control, coordination and judgment which may contribute to motor vehicle-related injuries and deaths. In addition, cannabis has demonstrated an effect on the adolescent’s developing brain and increases the risk of serious mental health conditions, including psychosis and greater likelihood of drug dependence in adulthood.3
Even though state policies only apply to cannabis use by adults, they may increase access among adolescents and also perpetuate decreased perception of harm from the drug.4 States with cannabis laws have been found to have higher marijuana use and lower perception of risks compared with states without cannabis laws. However, it is still unclear whether the increase in the trend of use is due to changing cannabis policies or due to preexisting trends and perceptions.5 A study conducted before and after marijuana legalization revealed that adolescent cannabis use increased from 2.0 to 4.1% in Washington but no significant difference in Colorado.6
In Colorado and Washington, there has been an increase in cannabis-related hospital visits in the pediatric population after commercialization of Marijuana.6 In the state of New York, where recreational cannabis was legalized on March 31 2021, there had been increasing reports of cannabis exposure, especially in children less than 5 years old.7 The primary objective of this study is to determine whether there is an increase in cannabis exposure in pediatric patients seen at the emergency department of a New York City Hospital after legalization of recreational marijuana.
METHODS
A single-center retrospective study, reviewed and approved by New York University Institutional Review Board (Protocol Number: s22-01514), was carried out in this study. Data were obtained from electronic medical records of a public city hospital in Brooklyn NY. Inclusion criteria were as follows: (1) pediatric emergency department encounters, (2) encounters from April 1 2019 to March 31 2023 (representing 2 years before and 2 years after legalization of recreational cannabis in the state of New York), (3) patients aged 0 - 18 years, and (4) patients with a urine drug screen positive for Tetrahydrocannabinol (THC), which served as the indicator of cannabis exposure in the study.
Demographic profile, chief complaint, diagnosis, comorbid psychiatric/developmental condition, other substances used, and patient disposition were obtained. Data were then summarized utilizing descriptive measures. Significance of difference between groups (before and after) were analyzed using Mann-Whitney U test and Chi-square test. Logistic regression was used to calculate odds ratio.
RESULTS
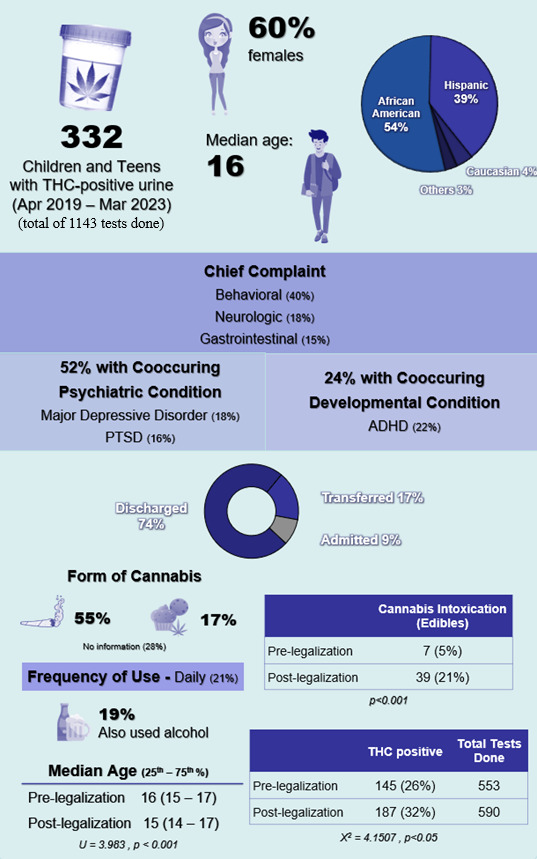
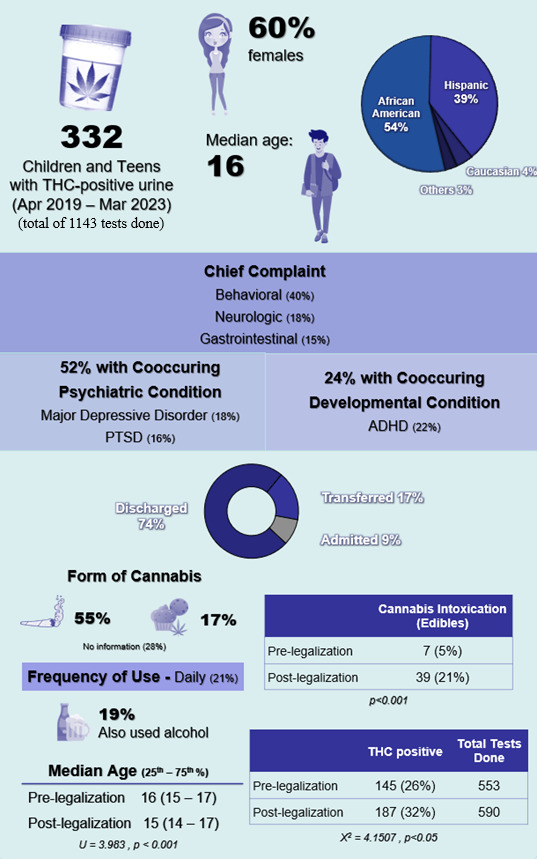
From a total of 1,143 urine drug screens done, 332 children and adolescents had THC-positive urine at the pediatric emergency department from April 2019 to March 2023. These urine drug screens were ordered based on clinical judgement, typically for suspected substance use involving one or more substances (not limited to cannabis) or to rule out substance exposure during the evaluation of symptoms as part of the differential diagnosis. Median age was 16 years old and the majority were females (60%). Most were African American (54%) or Hispanic (39%), reflecting the population catered by the hospital (Table 1). The most common chief complaints were behavioral (40%), neurologic (18%), and gastrointestinal (15%). Most cases were mild and were discharged home (74%).
Major depressive disorder (18%) and attention deficit hyperactivity disorder (22%) were the most common co-occurring psychiatric and developmental conditions (Table 1). Combustibles (55%) were the most common form of cannabis use followed by edibles (18%). And for those with documented frequency of use, daily use (21%) was the most common. Twenty-six percent (26%) concomitantly used other substances and alcohol (19%) was the most common.
THC positivity rate of urine drug screen increased from 26% (145 out of 553) to 32% (187 out of 590) before and after legalization of recreational cannabis. This increase was statistically significant (p<0.05).
Median age of children significantly decreased (p<0.001) from 16 to 15 years old (Table 1). Cannabis exposure among children 5 years and below slightly increased but was not statistically significant (positivity rate 25% vs 32%, p<0.738). However, children 5 years old and below were 10 times more likely to be hospitalized or transferred (OR 10.66, CI 95%, p<0.001) compared to older age group.
Cannabis related diagnosis (e.g. cannabis intoxication, cannabinoid hyperemesis syndrome, cannabis use) markedly increased from 14% to 36% (p<0.001). Furthermore, intoxication from cannabis edibles significantly increased from 5% to 21% (p<0.001). Despite these results, only 1 in 5 (18%) patients who tested positive for urine THC received on-site counseling and patient education on risks of cannabis use and/or its harmful effects.
DISCUSSION
Females had higher prevalence of cannabis use in our study. This finding is comparable with the recent trend from the latest National Youth Risk Behavior Survey (2021) and Monitoring the Future Survey (2023) regarding cannabis use in teens.8,9 Several factors may contribute to this pattern, including evolving social norms, increased perceived acceptability of cannabis use among adolescent females, and higher rates of internalizing symptoms such as anxiety and depression, which have been associated with cannabis use during adolescence.10 Nonetheless, the mechanisms underlying these sex-based differences remain unclear, and further research is needed to better understand the social, psychological, and contextual factors contributing to these trends.10 Combustible cannabis was also the most common type of product used by adolescents based on existing data.11 However, concerns exist regarding increasing use of alternative methods of cannabis, including vaping and edibles, due to perception of decreased risks from these products.11
Decreased perception of harm and increased accessibility of cannabis products in the pediatric population has been linked to legalization of marijuana.4,5 A recent study revealed an increasing trend of cannabis-involved emergency department visits in the youth after the COVID-19 pandemic and the associated expansion of state policies legalizing cannabis use.12 A finding that is comparable to our study - increase in THC detected in the urine of patients and increase in cannabis-related visits in our pediatric emergency department after legalization of recreational marijuana. Although most cases were mild, it is associated with increased healthcare burden and costs.
Multiple studies have also supported an increase in incidence of edible cannabis poisoning in children in the past few years.13–16 One particular study revealed a 1375% increase in pediatric cannabis exposure in a span of 4 years.16 This increasing trend of cannabis edible poisoning was also found in our study. It is quite alarming due to the significantly younger age group affected after legalization and increased hospitalizations in children below 5 years old. With the lack of nationwide laws to regulate packaging and potency of available cannabis products, children are disproportionately and negatively affected by the less stringent policies on adult cannabis use.
Beyond the influence of recreational cannabis legalization, several additional factors likely contribute to the observed rise in pediatric cannabis exposure. Recent literature has highlighted the significant impact of the COVID-19 pandemic on adolescent and family mental health, with increased stress, social disruption, and reduced access to routine support systems contributing to changes in substance use patterns.17,18 A New Jersey pediatric emergency department study reported that increases in cannabis use and exposure during this period were more strongly associated with pandemic-related psychological distress than with policy changes alone.19 Mental health and developmental vulnerabilities also play an important role, as up to half of the affected children in our study had psychiatric comorbidities such as major depressive disorder or post-traumatic stress disorder, and nearly a quarter had developmental conditions including ADHD. These underlying conditions are known to heighten impulsivity, emotional dysregulation, and susceptibility to self-medication, which may partly explain increased risk of intentional or unintentional cannabis exposure among youth.20,21
Equity considerations further contextualize these findings. This study noted that pediatric patients presenting with cannabis exposure are disproportionately African-American and Hispanic, reflecting not only local demographic patterns but also broader structural inequities that influence substance use risk. Factors such as socioeconomic disadvantage, limited access to preventive care, neighborhood stressors, and longstanding stigma surrounding behavioral health may delay help-seeking and contribute to unmet mental health needs in these communities.22 These intersecting vulnerabilities highlight that pediatric cannabis exposure is shaped by more than legalization alone; it is also influenced by mental health burden, family stress, and social determinants of health.23 Understanding these overlapping contributors is essential for developing targeted prevention strategies and for ensuring that public health efforts equitably reach populations at highest risk.
Legalization of recreational cannabis remains a relatively new phenomenon, and more research is required to fully understand its long-term impact on youth. Our study has several limitations that should be acknowledged. It was conducted at a single center, which may limit generalizability to other populations or geographic areas. In addition, we did not collect qualitative information on adolescents’ reasons for using cannabis, their perceptions of associated risks, or other contextual factors that may influence exposure. Finally, the study did not assess additional variables such as family stress, school disruptions, or broader community-level influences that could have contributed to changes in cannabis use during the study period. These limitations highlight the need for further investigation, including qualitative or mixed-methods studies, to better understand the experiences, motivations, and decision-making processes of youth and their families regarding cannabis use.
Addressing the negative implications of recreational cannabis legalization requires a comprehensive approach beyond policy and regulatory measures. While marketing and packaging regulations remain important, public health strategies should also focus on education campaigns that target both adolescents and their parents, community and school-based prevention programs, and psychosocial interventions that reduce vulnerability to substance use. Programs that strengthen family and community support systems, provide mental health resources, and are culturally responsive may be particularly effective for populations at higher risk.24,25 By combining regulatory safeguards with education and community-based interventions, public health efforts can more effectively prevent pediatric cannabis exposure and promote safer outcomes as legalization continues to expand.
CONCLUSION
While the legalization of recreational cannabis has led to increased accessibility and use among adolescents, it has also resulted in a troubling rise in cannabis-related health incidents, particularly among young children. Our study highlights the concerning trends of higher cannabis exposure among the pediatric population, the growing prevalence of cannabis-related emergency visits, and the alarming increase in edible cannabis poisonings in younger children. Despite the mild nature of many cases, the rising healthcare burden and potential long-term effects on youth demand urgent attention. As cannabis legalization continues to expand, it is crucial to implement stricter packaging and marketing regulations, alongside robust educational campaigns, to mitigate these risks and safeguard the health of future generations. More research is needed to fully understand the impact of cannabis legalization on public health, particularly within vulnerable pediatric populations, to ensure that policies evolve in ways that prioritize safety and well-being.
ACKNOWLEDGEMENTS
We would like to thank Mr. Anthony DiVittis and Ms. Bella Choa for providing statistical support in data analysis. We would also like to thank all the providers and nurses of Woodhull Hospital Department of Pediatrics for their dedication in caring for our patients.
ETHICAL STATEMENT
The study protocol (protocol reference #: s22-01514) adhered to the Declaration of Helsinki and was approved by the NYU Institutional Review Board.
DISCLOSURE STATEMENT
The authors report no conflict of interest
Positionality
The authors of this research are all pediatricians who have served the underserved urban pediatric population and witnessed the impact of substance use in the community. Our shared commitment to health equity and preventive care informs our desire to examine how legislation can shape pediatric outcomes and guide future policy and community interventions.
About the Authors
John Robyn Diez, MD
Dr. John Robyn Diez is an outpatient addiction medicine physician at Rural Western Maryland. He received his nursing and medical degree in the Philippines and then completed pediatric residency training at Woodhull Medical and Mental Health Center at Brooklyn NY. He also completed addiction medicine fellowship at The Ohio State University.
Prabhjot Sekhon, MD
Dr. Prabhjot Sekhon is a pediatric pulmonology fellow at NYP Morgan Stanley Children’s Hospital in NY. She completed her medical education in India and pediatric residency training at Woodhull Medical and Mental Health Center.
Aida Miyagusuku-Chang, MD
Dr. Aida Miyagusuku-Chang is a pediatric endocrinology fellow at UPMC Childrens Hospital at Pittsburgh PA. She completed her medical education in Peru and pediatric residency training at Woodhull Medical and Mental Health Center.
Rubina Maharjan, MD
Dr. Rubina Maharjan is a neonatology fellow at Children’s Mercy Hospital in Kansas City MO. She completed her medical education in Nepal and pediatric residency training at Woodhull Medical and Mental Health Center.
Marsha Medows, MD
Dr. Marsha Medows is the Associate Program Director of the pediatric residency program of Woodhull Medical and Mental Health Center. She is also a Clinical Assistant Professor in pediatrics at New York University Grossman School of Medicine.